Every tyranny perpetuates itself by indoctrinating the children. The Globalist destructocrats are following the same playbook. Is it too late for the children you care about? Too late for us?
Spoiler alert: this is a long post tying several threats together. I urge you to take the time to read it and share it as widely as you can. And join the Council of Concerned Citizens (C3) to, quite literally, end the deadly globalist control while the window of opportunity is still open.
“Give me a child until he is 7 and I will show you the man.”
Although widely attributed to the Greek philosopher Aristotle (probably apocryphally), Jesuit founder Ignatius of Loyola, Jesuit missionary St. Francis Xavier and philosopher mystic Rudolf Steiner, no one knows who first articulated the idea that a child is stamped indelibly by early conditioning, experiences, beliefs, rewards, successes and failures.
No normal human being who has cared for a young child has ever failed to notice the importance of those experiences, nor has any educator, nutritionist, doctor, psychologist, marketer, proselytizer or tyrant. Nor have the globalists.
Dr Rima Truth Reports Substack is paywall free and supported by our readers. To receive new posts and support my work, subscribe and support your health with amazing drug-free vibrotactic technology: DrRima.Superpatch.com.Subscribe
We all understand intuitively (probably because it is the truth of our own origins) that early learning/conditioning/programming/training/socialization is, in effect, a capture system of mind, body and spirit. For most of us, of course, that stimulates us to do our best to induce alignment with truth and positive values, both inner and outer, to sustain and support the life that will inevitably follow from the deep inner reality of those early years.
Lest we forget, mind control is a very real and powerfully corrosive tool of the globalist cabal, etching carefully crafted “reality” into the minds, hearts, bodies and souls of the denizens of their envisioned future world. In fact, through mind control and conditioning, we can be induced to believe, repeat and cling to, gibberish, illogic, rage and orchestrated destruction of ourselves and everything that sustains us.
War, for example, would be a pretty good example of that. Try this thought experiment for a moment: say out loud, “All wars are bankers’ wars”.
Now substitute the word “globalists” for “bankers”. Say it again, with the substitution: “All wars are globalists’ wars”. Next, insert the wars that are flaring or being readied, like this:
”All Gaza wars are globalists’ wars”,
“All illegal immigrant vs. ICE wars are globalists’ wars.”
“All bioweapon/gene therapy wars are globalists’ wars”,
“All gender ideology wars on children are globalists’ wars.”,
“All agricultural destruction wars on the food supply are globalists’ wars.”,
“All propagandemic wars on informed consent and personal rights are globalists’ wars.”.
“All weather modification wars on the planet and its inhabitants are globalists’ wars”.”Leave a comment
You get the idea. Nothing is by accident. For example,
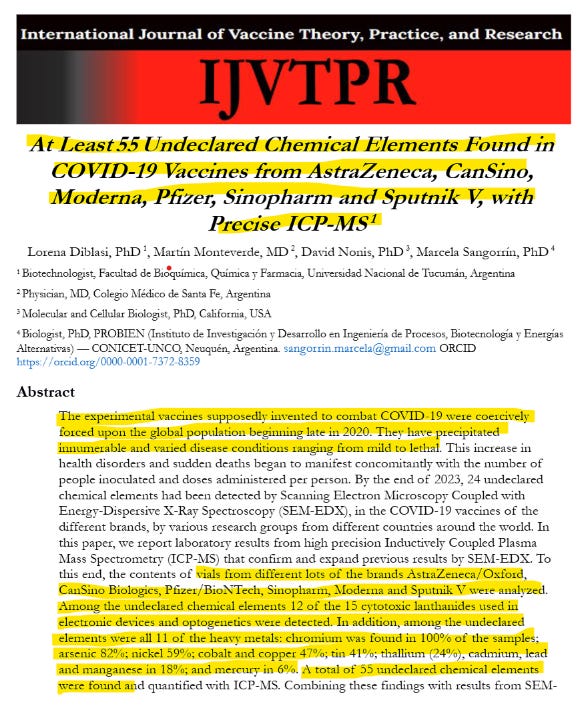
EVERY SINGLE COVID “vaccine”, from the US, UK, China, Russia, India, every single one of them contained heavy metals like Chromium (100% of the vials), arsenic (82% of the vials), 12 out of the 15 cytotoxic (cell-poisoning) lanthanides used in electronic devices and optogenetics (!)
Promethium, Pm, is radioactive. If these toxins are found in diverse lots of EVERY Covid jab from around the world, it is because they are intended to be there. By design. After all, bioweapons are not intended to be either safe for the recipients or effective in protecting their health. They are supposed to be safe for the deployers because they are disguised as something else and effective in weakening and killing their victims. The rest is propaganda and deadly deceit.
Dr Rima Truth Reports Substack is a paywall free publication. Your support makes this work possible. Purchase your professional quality supplements @discount at US.Fullscript.com/welcome/RLaibowSubscribe
Do all regular vaccines contain lanthanides? If they do, we can safely conclude that they are all intended to cause biological chaos, as part of the war on our health and survival. If they do not, and available information would suggest that they do not, it must be assumed that since ALL of the Covid jabs contain them, it is by design.2 Do all vaccines contain heavy metals? In fact, many do contain mercury and most contain aluminum. So, we can safely conclude that they are all intended to cause biological chaos, as part of the war on our health and survival.
All wars are globalists’ wars.
And the globalists are proven themselves over the ages more than eager and willing to dispose of huge numbers of us at their whim, bringing the rest of us to destitution and misery at their pleasure and profit. Nothing has changed.
A note here about ascribing racial, religious or political identities to these monstrous traitors to humanity. They have no nationality, religion or affiliation to any of the things that move and motivate us. Their only affiliation is to their own psychopathic perceived good. They are not Jewish monsters, or Catholic monsters or German monsters or white monsters or Zionist monsters or colonialist monsters or Marxist monsters. They are monsters whose ONLY identify is as centers of power and wealth, whatever it costs us. It is important to recall that, to the globalists, the divisions that matter so much to us, race, nations, religions, economic systems, political systems, ethnic heritage, human rights and needs, matter not at all. We need to see beyond those divisions in order to see them at all, in fact.
There is, after all, a reason that so many people were so readily manipulated into believing irrational nonsense re: COVID, bioweapons dressed up as vaccines, lockdowns, masks as barriers to viruses, and on and on and on, to say nothing of, for instance, massive steel and concrete skyscrapers crashing down in their own footprints when struck by an airplane (WTC 1, 2) or not (WTC 7) with surviving passports and all.
This programming has been going on for a very, very long time. And it is still going on, right now, today, with high-level intensity in our schools, just as well as in our world.
Once again, Connie Shields has written compellingly about the “Look Over There” Davos theater while something very important, and largely unnoticed, was going on. Here is her outstanding substack:
I think there is, however, more to the Davos theatrical production than Mark Carney’s absurd “Power of the Powerless” “Us medium sized guys ain’t gonna get pushed around by those big hegemons no more! No sir! We got us some powerful new rules now and we are, by God, gonna use ‘em!”3 and Donald Trump’s ridiculous cult of personality “I’m big and I’m scary tough and I got some serious superpowers you ain’t even dreamed about, and I’m gonna take what I want because I can and you should be grateful that’s all I’m taking because you and your puny little runt brothers couldn’t stop me if you tried!”4
Here’s what I think is going on, including my predictions for what we will see on the national and international scene in the next several months:
Davos and the entire geopolitical Venezuela/Greenland/Cuba/…. expansion by the US, is carefully scripted. The cartoon character roles have been assigned: Carney, the consummate globalist, Macron, his clearly controlled sidekick, and Trump, desperate to be the beloved populist hero, but secretly serving the globalist agenda (No? have you forgotten Operation Stargate?) Their job at Davos is to pretend to be in a huge squabble over which forces control the world while cementing the actual hegemony of the Globalist cabal.
The US could set up as many bases as it likes in Greenland without seizing it. The Greenland grab is designed not to protect anyone, but to fracture NATO.
The Venezuelan kidnap of a sitting President and essential confiscation of its rich and valuable resources is not about oil, of which the US has plenty. It is designed, along with the coming capture of Cuba and possible seizure of other Caribbean, South and Central American territories, to shatter the trade and military alliances and allegiances that function similarly to the way that NATO and trade agreements do in Europe.
The US is putting out the preparatory propaganda to seize control of Cuba next.
I predict some sort of emergency-based “need” will arise in the next few months ‘forcing” the US to commandeer, seize, annex, capture or otherwise take control of someplace in the Pacific. Okinawa? Taiwan? Tasmania?” New Zeeland? Islands in the South China Sea? the Philippines? Someplace needs to be seized to destroy the same class of alliances: military and economic. Of course, right now all the land in the Pacific actually belongs to other sovereign nations but never mind that. We have moved Back to the Future into the era of the New Monroe Doctrine and the gunboat diplomacy of 21st Century weapons, rather than 19th Century ones.
While all of this is going on, the United Nations will play its part as the old, feeble, inept and laughable dotard whose hold on power has slipped so he needs to be replaced by the young, heroic and dashing figure who emerges out of the chaos of the breakdown of the old order.
In this case, it is likely to be the heroic, larger-than-life, revitalized and reinvigorated US swooshing in with a New [WORLD] Order, the Board of Peace which is not like the UN at all!
It is not corrupt like the UN. No Siree!
It is not impotent like the UN. Not even a little bit! Good ol’ US Can Do at work!
It is not the plaything of the shockingly wealthy individuals and corporations serving the money system like the UN does. You betcha it stands ready to defend truth, justice and the common man!
It is based on our shared values, with wealth shared among those who can hold onto it best. That way the worthiest get the most!
It is based on might, which generates automatic right! That’s the American Way, per the modern version of the Monroe Doctrine, after all! See above!
So, this swashbuckling hero gets to put a fresh new face on the same old, same old globalist tyranny.
And this is pretty dim and grim except…. This power vacuum is a shining opportunity for us, right now.
The disruption so carefully scripted opens up the possibility for a different reorganization to be superimposed on the one the power brokers have in mind. History is full of moments where the intended outcome of a disruption turned out to be quite different.
And that is what this carefully scripted theatrical gong show offers us: As the UN-dominated hegemony is replaced with the next iteration, We, the People, swoop in and lean very, VERY heavily on Congress to do what we, in our massive numbers, force them to do:
Amend the Disengaging Entirely From the United Nations Debacle Act of 2025 (now before both the House and the Senate) to require unwinding all UN Regulatory Capture at every level of governance and
Prohibit the US from participating in any organization or structure with the potential to become a world government.
Once those amendments are in place, Congress must pass the bill and, as it already requires, exist the UN and eject all of its parts from our shores. Executing effective removal of the UN’s Regulatory Capture is the working end of this bill since membership in the organization is no longer significant, now that it has captured our professions, economy, municipalities, regulations, education, transportation and freedom of speech. Clearly, eliminating the Regulatory Capture, and detoxing from the UN parasitic infestation we are being consumed by is essential. That’s why we are asking for as many people as possible to join the Council of Concerned Citizens (C3). Learn more here: Join C3 here:
“…The multilateral institutions on which the middle powers have relied — the WTO, the UN, the COP, the very architecture of collective problem-solving — are under threat. As a result, many countries are drawing the same conclusions that they must develop greater strategic autonomy in energy, food, critical minerals, in finance and supply chains. And this impulse is understandable.
A country that cannot feed itself, fuel itself or defend itself has few options. When the rules no longer protect you, you must protect yourself.
But let’s be clear-eyed about where this leads. A world of fortresses will be poorer, more fragile and less sustainable.
And there’s another truth: if great powers abandon even the pretense of rules and values for the unhindered pursuit of their power and interests, the gains from transactionalism will become harder to replicate.
Hegemons cannot continually monetize their relationships. Allies will diversify to hedge against uncertainty. They’ll buy insurance, increase options in order to rebuild sovereignty — sovereignty that was once grounded in rules but will increasingly be anchored in the ability to withstand pressure…..” Read the full transcript of Carney’s speech to World Economic Forum – National | Globalnews.ca
“…After the war, we gave Greenland back to Denmark. How stupid were we to do that? But we did it, but we gave it back. But how ungrateful are they now? So now our country and the world face much greater risks than it did ever before, because of missiles, because of nuclear, because of weapons of warfare that I can’t even talk about.
Two weeks ago, they saw weapons that nobody ever heard of. They weren’t able to fire one shot at us. They said, ‘What happened?’ Everything was discombobulated. They said, ‘We’ve got them in our sights. Press the trigger.’ And nothing happened. No anti-aircraft missiles went up. There was one that went up about 30 feet and crashed down, right next to the people that sent it. They said, ‘What the hell is going on those?’ Those defensive systems were made by Russia and by China. So, they’re going to go back to the drawing boards, I guess.
Greenland is a vast, almost entirely uninhabited and undeveloped territory, sitting undefended in a key strategic location between the United States, Russia and China. That’s exactly where it is, right smack in the middle. Wasn’t important, nearly, when we gave it back. You know, when we gave it back, it wasn’t the same as it is now. It’s not important for any other reason. You know, everyone talks about the minerals, there’s so many places… There’s no rare earth. No such thing as rare earth. There’s rare processing, but there’s so much rare earth, then to get to this rare earth, you have to go through hundreds of feet of ice.
That’s not the reason we need it. We need it for strategic national security and international security. This enormous unsecured island is actually part of North America, on the northern frontier of the Western Hemisphere. That’s our territory. It is therefore a core national security interest of the United States of America, and in fact, it’s been our policy for hundreds of years to prevent outside threats from entering our hemisphere, and we’ve done it very successfully. We’ve never been stronger than we are now.
That’s why American presidents have sought to purchase Greenland for nearly two centuries. You know, for two centuries they’ve been trying to do it. They should have kept it after World War Two, but they had a different president. That’s all right, people think differently. Much more necessary now than it was at that time.
However, in 2019 Denmark said that they would spend over $200 million to strengthen Greenland’s defences. But as you know, they spent less than 1% of that amount, 1%. No sign of Denmark there. And I say that with great respect for Denmark, whose people I love, whose leaders are very good.
It’s the United States alone that can protect this giant mass of land, this giant piece of ice, develop it and improve it, and make it so that it’s good for Europe, and safe for Europe, and good for us. And that’s the reason I’m seeking immediate negotiations to, once again, discuss the acquisition of Greenland by the United States – just as we have acquired many other territories throughout our history. As many of the European nations have, they’ve acquired. There’s nothing wrong with it. Many of them. Some went in reverse, actually, if you look. Some had great, vast wealth, great, vast lands, all over the world. They went in reverse. They stuck back where they started. That happens too, but some grow.
But this would not be a threat to NATO. This would greatly enhance the security of the entire alliance, the NATO Alliance. The United States is treated very unfairly by NATO. I want to tell you that. When you think about it, nobody can dispute it. We give so much, and we get so little in return. And I’ve been a critic of NATO for many years, and yet I’ve done more to help NATO than any other president, by far than any other person. You wouldn’t have NATO if I didn’t get involved in my first term….” Davos 2026: Special Address by US President Donald J Trump | World Economic Forum
Government preparation for large-scale mRNA vaccination of livestock.
Chinese government–funded researchers have confirmed that they tested an mRNA bird flu vaccine in lactating dairy cows, injecting milk-producing livestock with an mRNA–lipid nanoparticle formulation and then deliberately exposing the animals to live H5N1 influenza virus inside high-containment laboratories.
The peer-reviewed study published on Monday, in the journal Research, is titled “Protective Efficacy of a Hemagglutinin-Based mRNA Vaccine Against H5N1 Influenza Virus Challenge in Lactating Dairy Cows.”
The experiment signals that governments are actively preparing mRNA platforms for potential large-scale use in livestock populations, extending mRNA deployment beyond humans and into the food supply.
mRNA Vaccine Administered to Food-Producing Animals
According to the study, researchers injected an mRNA vaccine into lactating Holstein dairy cows, meaning animals actively producing milk.
The authors write:
“Six healthy lactating dairy cows were intramuscularly immunized with 500 μg of the mRNA vaccine twice, with a 3-week interval between doses.”
The animals were sourced from an external farm:
“Lactating Holstein cows, 3 to 5 years of age, obtained from a local dairy farm, were used in the challenge experiment.”
The vaccine was an mRNA–lipid nanoparticle (mRNA–LNP) formulation encoding the hemagglutinin protein of an avian influenza virus:
“We developed a monovalent, cattle-codon-optimized mRNA–LNP vaccine encoding the HA protein.”
Deliberate Infection with H5N1 Pathogen
After receiving the mRNA injections, both vaccinated and unvaccinated cows were moved into animal biosafety level 3+ (ABSL-3+) laboratories and deliberately infected with a purportedly live H5N1 influenza virus.
The paper states:
“3 vaccinated and 3 unvaccinated lactating dairy cows were transferred into the animal biosafety level 3+ (ABSL-3+) facility for the challenge study.”
The virus was said to be administered through multiple routes, including direct injection into the mammary glands:
“All cows received a DC/24 virus challenge administered via both the intranasal and intramammary routes.”
The authors further specify:
“3 doses were directly inoculated into separate mammary quarters via the teat.”
All work involving the pathogen was performed inside Chinese state-authorized high-containment laboratories.
The methods section states:
“The procedures involving live HPAI viruses were performed within certified BSL-3 and ABSL-3+ laboratories at the Harbin Veterinary Research Institute (HVRI), Chinese Academy of Agricultural Sciences (CAAS).”
The H5N1 viruses used were not simple field samples but laboratory-generated strains.
The authors cite a prior peer-reviewed study for the virus’s creation and laboratory handling methods, rather than detailing the generation process in this paper.
“The challenge dairy cow H5N1 virus (DC/24)… was generated as previously described.”
Chinese Government Funding
The study was funded entirely by Chinese state and government research programs.
The funding disclosure reads:
“This research was funded by the National Key Research and Development Program of China… the National Natural Science Foundation of China… the Innovation Program of the CAAS… the natural science foundation of Heilongjiang Province… [and] the Central Public Interest Scientific Institution Basal Research Fund.”
All authors are affiliated with Chinese government research institutes or state-linked laboratories, including the Chinese Academy of Agricultural Sciences and China’s National High Containment Laboratory for Animal Disease Control and Prevention.
Bottom Line
The paper confirms that China is now testing mRNA vaccine platforms directly in livestock, including milk-producing animals, using live avian influenza viruses under high-containment laboratory conditions.
The study documents the use of modern mRNA technology not only in humans or laboratory animals, but in food-supply species that interface directly with agriculture, trade, and public health systems.
A closed pandemic loop of digital design, synthetic GOF viruses, and government-controlled verification.
A new peer-reviewed study published in the journal Viruses says that publicly funded Canadian laboratories digitally designed full-length SARS-CoV-2 genomes, chemically synthesized them using commercial services, and generated live, replication-competent coronaviruses without starting from a natural virus sample.
The paper, titled “Developing Synthetic Full-Length SARS-CoV-2 cDNAs and Reporter Viruses for High-Throughput Antiviral Drug Screening,” documents the alleged creation of infectious Delta and Omicron SARS-CoV-2 viruses from computer-designed genetic sequences alone.
Coming in the wake of the COVID-19 pandemic—which killed millions of people worldwide and was linked by multiple intelligence agencies to laboratory research—the study raises national security concerns about the ability of government-funded institutions to create replication-competent pandemic viruses from digital sequence data alone, using commercial infrastructure with limited public oversight.
In light of these capabilities, the study also raises the possibility that governments could define, simulate, and respond to a biological threat almost entirely within digital and laboratory frameworks—leaving the public reliant on official interpretation rather than independently observable evidence.
Viruses Built from Computer Code Alone
The authors state that they did not rely on physical viral isolates to create the viruses.
Instead, they used commercial DNA synthesis services to generate the entire coronavirus genome:
“We opted to use cDNA chemical synthesis services to generate full-length wild-type and reporter Delta and Omicron clones.”
They further explain:
“DNA synthesis is a viable method to rapidly generate coronavirus cDNAs and recombinant viruses.”
Those synthesized genomes were then said to be used to generate live viruses:
“Clone-derived Delta and Omicron wild-type and reporter viruses were successfully rescued and showed replication kinetics comparable to patient-derived isolates.”
The study claims that the resulting viruses were infectious and capable of sustained replication in cell culture.
The paper emphasizes that the same system can be used to generate new viral variants based solely on sequence data:
“DNA synthesis is a viable and rapid option to generate reverse genetic systems for wild-type and reporter viruses using sequence information alone.”
Acknowledged Gain-of-Function Capability
In the Discussion section, the authors explicitly acknowledge that the methodology they used qualifies as gain-of-function (GOF) capable research:
“It is important to acknowledge that the novel approach described in this study—generating replication-competent viruses from synthetic DNA while introducing heterogeneous gene functions—can be used for ‘gain-of-function’ research.”
Where the Viruses Were Said to Be Created
All work involving purportedly live SARS-CoV-2 was conducted in Canada at a high-containment facility:
“All the experiments involving infectious SARS-CoV-2 viruses were conducted at VIDO-InterVac in an approved Biosafety containment level 3 (BSL3) laboratory.”
VIDO-InterVac is part of the University of Saskatchewan, which is a central institutional hub for the research described in the paper.
Author Affiliations
The authors are affiliated with multiple Canadian institutions, including:
University of Saskatchewan (Department of Biochemistry, Microbiology, and Immunology; Vaccine and Infectious Disease Organization),
University of Alberta (Department of Cell Biology; Department of Medical Microbiology & Immunology; Li Ka Shing Institute of Virology),
Sunnybrook Research Institute (Toronto),
University of Toronto (Department of Laboratory Medicine and Pathobiology).
Public Funding Sources
The research was funded entirely through public Canadian funding, according to the paper’s funding disclosure:
“This research was funded by the Canadian Institutes of Health Research (CIHR)-funded Coronavirus Variants Rapid Response Network (CoVaRR-Net)… CIHR Operating COVID-19 Rapid Research Funding Opportunity—Therapeutics… and NSERC.”
Additional operational support came from:
“The Government of Saskatchewan… the Government of Canada through Prairies Economic Development Canada… and the Canada Foundation for Innovation Major Science Initiatives for its CL3 facility.”
What the Paper Establishes
The study documents, in the authors’ words, that:
Full-length SARS-CoV-2 genomes were digitally designed
Those genomes were chemically synthesized
Live, replication-competent coronaviruses were said to be generated from that synthetic DNA
The method is acknowledged to be usable for gain-of-function research
The work was publicly funded and conducted in Canadian government-supported laboratories
These facts are stated directly in the paper and do not rely on inference, speculation, or external interpretation.
Bottom Line
The new Viruses paper reveals that governments claim to possess the technical ability to define a virus digitally, synthesize it physically, and validate its behavior entirely within controlled laboratory systems—allowing modern pandemic response to operate almost entirely inside digital, synthetic, and laboratory environments.
That convergence raises unresolved questions about national security, transparency, independent verification, and how much trust the public is asked to place in closed scientific and governmental frameworks when responding to future biological threats.
The study aligns with earlier FOIA-released DARPA documents showing that U.S. biodefense systems were already built to synthesize viruses and manufacture mRNA countermeasures from sequence data alone, placing the Canadian work within a broader pre-existing digital pandemic infrastructure.
Despite claiming to have withdrawn from the international organization.
Despite claiming to have formally withdrawn from the World Health Organization (WHO), the Trump administration has confirmed it is still in active discussions with the agency about participating in next year’s global influenza vaccine strain-selection process—at the same time the U.S. government is funding influenza bird flu gain-of-function research and a $500 million influenza vaccine initiative.
On January 22, the U.S. Department of Health and Human Services (HHS) announced that the United States had completed its withdrawal from the WHO, apparently ending all funding, recalling U.S. personnel, and terminating participation in WHO committees, governance bodies, and technical working groups.
During the same briefing, administration officials acknowledged that influenza remains an open channel for engagement.
“HHS left the door open to some continued collaboration, however. Asked if the US would participate in an upcoming WHO-led meeting to decide the composition of next year’s flu vaccines, the administration said conversations about that are still ongoing.”
The statement was made during a call with reporters following the withdrawal announcement.
This places influenza in a separate policy category—one where U.S. withdrawal exists on paper, but coordination with the same international decision system continues.
It raises questions about who is actually setting U.S. influenza policy, and why the one disease tied to global strain forecasting, pandemic modeling, and mass countermeasure production remains exempt from the break.
WHO Exit With Influenza Carve-Out
HHS stated the U.S. has:
Terminated all WHO funding
Recalled all personnel and contractors
Ceased participation in WHO technical working groups and governance bodies
Yet the administration declined to rule out involvement in the WHO’s influenza strain-selection process, which determines the purported viral lineages used in seasonal vaccines worldwide and shapes pharmaceutical manufacturing timelines.
Domestic Influenza Programs Continue to Expand
While negotiating ongoing coordination with the WHO, the federal government is simultaneously expanding influenza and bird flu research and vaccine programs inside the United States.
In 2025, HHS launched a $500 million federal influenza vaccine initiative described as a “gold standard” program designed to accelerate strain updates, enable rapid manufacturing, and support pre-pandemic deployment.
Federal agencies including the NIH, NIAID, USDA, and the Department of Defense continue funding laboratory research on avian and human influenza viruses that deliberately alter viral properties for study, including:
receptor binding changes,
mammalian transmissibility modeling,
chimeric viral backbones,
immune escape features.
These experiments are described in peer-reviewed publications and supported through federal research grants and biodefense contracting mechanisms.
U.S. agencies are also funding H5N1 bird flu vaccine platforms using reverse-genetics systems, chimeric viral constructs, and self-amplifying RNA technologies intended for pandemic countermeasure development.
Integrated Influenza Infrastructure
The WHO coordinates global influenza surveillance and strain forecasting.
The U.S. continues negotiating technical access to that system.
Federal agencies fund laboratory modification of influenza viruses and parallel vaccine platforms.
Pharmaceutical manufacturing and preparedness planning rely on the same surveillance and strain data.
Taken together, these disclosures show that despite the publicized WHO withdrawal, the United States remains functionally embedded in the WHO-centered influenza system—where global strain selection, federally funded virus engineering, and government-backed vaccine platforms converge inside the same international pandemic planning architecture.
Despite claims the U.S. has stopped bankrolling gain-of-function experiments.
A new peer-reviewed study published this week states that federally funded researchers genetically engineered viruses that gained biological functions not present in any naturally occurring strain, including new host-entry mechanisms, cross-species antigen display, and mammalian lethality.
In multiple cases, viral surface proteins from one species and virus family were deliberately inserted into the genetic backbone of an entirely different virus, creating laboratory chimeras that bridge species and viral lineages that do not naturally mix.
The paper, “Immunogenicity and Efficacy of a Rabies-Based Vaccine against Highly Pathogenic Influenza H5N1 Virus,” appears in Emerging Microbes & Infections.
The study documents three distinct categories of functional gain:
transfer of influenza entry machinery into foreign viral backbones,
reprogramming of rabies virus to perform influenza functions, and
creation of new influenza chimeras that are lethal in mammals.
(Editor’s note: This article makes no claims about virology and/or terrain theory. It is reporting what NIAID-funded scientists claim to be doing with American taxdollars.)
Funding & Research Sites
The authors state:
“This study was supported by… the Center for Research on Influenza Pathogenesis and Transmission (CRIPT), one of the National Institute of Allergy and Infectious Diseases (NIAID) funded Centers of Excellence for Influenza Research and Response (CEIRR; contract # 75N93021C00014), and by NIAID contract SEM-CIVIC (contract number 75N93019C00051).”
This raises national security and conflict of interest concerns, as it represents the simultaneous creation of a lucrative problem and solution.
NIAD is under the authority of U.S. Health and Human Services (HHS), which is led by Robert F. Kennedy Jr.
Animal experiments were approved under:
“the Institutional Animal Care and Use Committee (IACUC) of Thomas Jefferson University (TJU).”
Influenza Host-Entry Functions Transferred Into a Different Virus
The authors state that they created a vesicular stomatitis virus whose native entry protein was replaced with influenza H5:
“VSV∆G-H5-GFP encoding either the clade 1 H5 (A/Viet Nam/1203/2004(H5N1) or the circulating clade 2.3.4.4b cow was generated as described.”
This describes a virus that now uses influenza hemagglutinin to enter host cells—a function VSV does not naturally possess.
It also represents a direct cross-species and cross-virus transfer of host-entry machinery, merging an avian influenza protein with a livestock-associated strain and a human-infecting viral backbone in a single engineered system.
Rabies Virus Reprogrammed to Display & Deliver Influenza Antigen
The study confirms that a rabies virus was engineered to express influenza H5:
“We developed a rabies virus-based H5 vaccine (RABV-H5) by insertion of a synthetic full-length codon-optimized HA ORF of the Influenza virus A/Vietnam 1203/2004(H5N1) into the BNSP333 rabies vaccine vector between the N and P genes.”
The authors further state:
“Presenting both RABV-G and the antigen of choice on the surface.”
This confirms that a neurotropic virus was genetically modified to perform a new influenza-specific function.
The lab construct combines a mammalian neurotropic virus with an avian influenza surface antigen, creating a synthetic cross-species hybrid that does not exist in nature.
Creation of Novel Influenza Viruses That Did Not Exist in Nature
The paper says that new influenza viruses were constructed by genome segment replacement:
“PR8-H5N1, a recombinant Puerto-Rico 8 influenza A virus (A/PR8) in which the HA and NA genomic segments have been replaced with the respective segments of H5N1.”
The authors report intranasal infection of mice with the engineered viruses:
“On days 104 or 150, mice were challenged by IN instillation with 0.05 ml of either 1E5 TCID50 of Influenza A/PR8-H5N1 (Viet Nam 1203 or Cow) or with 100 pfu of HPAI-H5N1 Viet Nam 1203 (2004) diluted in PBS+1% heat-inactivated FBS.”
They further confirm the dose was lethal:
“[O]n day 104 were challenged by IN instillation with a 1E5 pfu lethal dose of A/PR8-H5N1 Viet Nam 1203 virus (>100LD50).”
The paper documents viral replication in lungs:
“While unvaccinated mice had about 1E6 TCID50/ml of replicating virus in the lungs.”
And describes lung pathology:
“Severe and chronic bronchiolocentric infection with bronchiolar and peribronchiolar infiltration of lymphocytes, associated with interstitial pneumonitis and expanded alveolar wall due to edema and inflammation.”
Bottom Line
The new study makes clear that gain-of-function virus creation is allegedly still being carried out with U.S. taxpayer dollars, despite the national security and biosafety risks such work poses to the very population funding it.
On Wednesday, the World Health Organization (WHO) published an influenza fact sheet in which it declared that influenza pandemics are on the horizon, emphasizing bird flu.
It did not say a future pandemic is a possibility.
The unelected foreign organization stated its coming is a fact, writing:
There will be influenza pandemics in the future, but when and with which virus, as well as where and how they will spread, is difficult to predict. They can have significant health, economic and social consequences. An influenza pandemic arises when an influenza virus emerges with the ability to cause sustained human-to-human transmission, and the human population has little to no immunity against the virus.
Whether currently circulating avian, swine and other influenza viruses will result in a future pandemic is unknown. However, the diversity of zoonotic influenza viruses that have caused human infections necessitates strengthened surveillance in both animal and human populations, thorough investigation of every zoonotic infection and pandemic preparedness planning.
The WHO financially benefits from pandemics.
The org received approximately $7.9 billion in total funding during the 2020-2021 biennium, exceeding its $5.84 billion approved budget by 36% due to massive COVID-19 emergency contributions.
Of this, around $3 billion was specifically for COVID-19 operations, marking an unprecedented surge from pre-pandemic levels.
A top contributor to the WHO is Bill Gates, who recently—through his Coalition for Epidemic Preparedness Innovations (CEPI)—invested $54.3 million to support Moderna’s new mRNA-based pandemic H5 avian influenza “bird flu” vaccine candidate, mRNA-1018.
If the WHO’s pandemic warnings are being issued inside a funding ecosystem that profits from crisis response—while those same donors bankroll laboratories now linked by governments to pandemic creation and fund programs that deliberately infect Americans with lab-grown influenza—then the line between public health forecasting and systemic orchestration is no longer defensible.
Gates Foundation Trust holds hundreds of millions of dollars in companies like Chevron, BP, and Shell while simultaneously investing in climate change initiatives—profiting from both ends.
The Gates Foundation Trust has invested hundreds of millions of dollars in oil extractors despite Bill Gates’ claims that the industry is to blame for long-debunked “climate change,” according to a Monday report from The Guardian.
The new report confirms:
“End-of-year filings reveal that in 2024 the trust invested $254m in companies that extract fossil fuels such as Chevron, BP and Shell. This was a nine-year record and up 21% from 2016, Guardian analysis found. Adjusting for inflation, it was the highest amount since 2019.”
Gates has claimed that Big Oil products are making the future “worse” for humanity.
“[B]urning fossil fuels helps people now at the cost of making the climate worse for people in the future.”
This raises logical questions:
If fossil fuel extraction, in Gates’ opinion, makes the future worse for humanity, why is the Gates Foundation Trust investing over a quarter of a billion dollars in the very industry Gates publicly condemns?
Why does Gates urge the world to divest from fossil fuels while his own trust quietly profits from them?
Why is oil framed as a moral threat to humanity—yet treated as a lucrative investment when Gates’ money is on the line?
Why is the public told to abandon fossil fuels while the Gates Foundation Trust expands its financial stake in them?
Why are ordinary people expected to sacrifice their livelihoods and energy security, while Gates’ foundation continues to profit from the same industry?
His investment strategy shows he is financially exposed to the very market failure he publicly defines as an existential threat—while also holding positions in the policy and technology sectors built to “fix” it.
In December, the Gates Foundation announced a four-year, $1.4 billion investment in “climate resilience.”
The same crisis Gates warns will destabilize the future is embedded in his trust’s revenue stream, with profits tied both to fossil fuel extraction and to the industries positioned as replacements.
The trust’s portfolio reflects a system where Gates benefits regardless of outcome: continued oil dependence or forced energy transition.
The financial record shows that the “problem” and the “solution” are not separate markets for Gates—they are part of the same revenue cycle.
Rather than distancing himself from the industry he condemns, Gates’ trust remains structurally dependent on it while also financing the mechanisms designed to dismantle it.
The record shows a closed financial loop in which the same actor who defines the worldwide threat is positioned to collect returns from both the continuation of that threat and the systems built to manage, regulate, and replace it.
Animals that ingest the oral vaccine are said to be contagious to other animals and humans for over a month.
On January 6, 2012, Brig. Gen. William L. Smith, Director Joint Staff and Commander, Domestic Operations for Joint Force Headquarters of Texas (second from left) met with members of the Texas State Guard and received an overview of the annual Texas Oral Rabies Vaccination Program in Zapata, Texas. Since the program’s inception in 1995, more than 39 million doses of the oral rabies vaccine, Raboral V RG, have been distributed over approximately 540,000 square miles of Texas. (U.S. Army Photo photo by Laura L. Lopez/Wikimedia Commons).
The Texas Department of Health and Human Services (DHS) has begun its annual distribution of RABORAL V-RG®, an oral rabies vaccine (ORV) bait—dropping the live laboratory-made virus from airplanes over Texas, as well as distributing it by hand.
The $2 million annual project is funded by the State of Texas and the United States Department of Agriculture Animal and Plant Health Inspection Service/Wildlife Services.
The U.S. Centers for Disease Control and Prevention (CDC) has known for over a decade that the RABORAL edible vaccine leaves “persons at risk for vaccine exposure and vaccine virus infection.”
Yet the department still allows millions of live genetically modified virus baits to be dispersed over communities, forests, and waterways each year without public notice, informed consent, or comprehensive biosafety oversight—posing potential risks to human health, wildlife, and national biosecurity.
Americans are being involuntarily exposed to laboratory-engineered pathogens capable of infecting multiple species, with no transparent risk disclosure or opt-out mechanism.
Texas Department of State of Health Services will expand anti-rabies efforts around the El Paso area in January during the agency’s 32nd annual Oral Rabies Vaccination Program. Aerial bait distribution, which occurs along much of the Texas-Mexico border, was increased last year to include far West Texas as a response to the Arizona Fox rabies variant that is now established in New Mexico and within 150 miles of the Texas border.
In addition to those continued flights this year, rabies vaccine baits will also be distributed by hand in targeted areas around the city.
The rabies vaccine bait air drop will begin with flights from Alpine on Jan. 16, with additional flights slated to originate from Del Rio International Airport on Jan. 21, weather permitting. The vaccine bait, manufactured by Boehringer Ingelheim Animal Health USA Inc., is enclosed in a small plastic packet (similar to a fast-food ketchup package) dipped in fish oil and fish-meal crumbles to attract wild canids, like coyotes and foxes.
Between six and nine flights are scheduled per day during the two-week operation, with airdrop aircraft flying at 500 to 1,000 feet above ground level and dropping roughly 693,600 oral rabies vaccine baits at 50 baits per square mile. ORVP’s Border Maintenance Zone includes 19 Texas counties including El Paso, Hudspeth, Culberson, Jeff Davis, Presidio, Brewster, Pecos, Terrell, Val Verde, Kinney, Maverick, Zavala, Dimmit, Webb, Zapata, Starr, Hidalgo, Cameron and Willacy.
In addition to the hand-distribution efforts in the El Paso area, baits will also be distributed by hand in parts of Cameron, Hidalgo, Starr and Willacy counties.
The U.S. Department of Agriculture warns humans “should leave [the live-virus containing edible vaccine] undisturbed if they are encountered.”
If people come in contact with the bait, “they should immediately wash the contact area with warm water and soap.”
Dogs that consume the bait “may experience a temporary upset stomach.”
A July 2019 peer-reviewed study in Vaccineconfirms the RABORAL oral rabies vaccine:
is a genetically engineered chimeric “Frankenstein” human virus expressing a rabies gene,
sheds for weeks in multiple species,
was not tested for live virus persistence,
can potentially infect non-target animals and humans,
and was studied by researchers financially tied to its sale.
Most alarmingly, the study confirmed that virus DNA from the edible vaccine can be detected in both oral and rectal swabs post-inoculation in most animals, “followed by a resurgence of shedding between days 17 and 34 in some species.”
This means animals that ingest the oral vaccine are said to be contagious to other animals and humans for over a month.
On January 6, 2012, Texas State Guard member, Private Paul Pettit of the 3rd Battalion, 1st Regiment takes part in one of the many flights that assists in the aerial distribution of Raboral V RG, during a 10-day Oral Rabies Vaccination Program. With statistics showing a drastic reduction in rabies cases the goal of this program is to create zones of vaccinated coyotes and gray foxes along the leading edges of the epizootics stopping the spread of the virus. (U.S. Army photo by Laura L. Lopez/Wikimedia Commons).
A September 2017 Veterinary Research publication confirms that the live virus in RABORAL edible vaccines actively replicates in animals after ingestion, that horizontal transmission of the vaccine virus between animals has occurred, and that humans have been infected with vaccine-derived vaccinia following bait exposure.
The same study shows that RABORAL baits deliberately disperse tetracycline—a toxic ingredient in the vaccine—into the environment as a biomarker, where it accumulates in animal bone and teeth, can misrepresent true vaccination, and is acknowledged to carry potential ecotoxicity and antimicrobial-resistance risks with long-term use.
In the name of “wildlife management,” Texas authorities are blanketing cities with what are said to be live virus-containing packets without full public consent.
How many Texans have been informed that they are living inside an ongoing, state- and federally funded environmental release of a live, laboratory-engineered virus documented to replicate, spread between animals, persist in bodily secretions, and infect humans—without informed consent or any meaningful ability to refuse exposure?
NIH, NIAID, and CRD directors refuse to halt deadly pathogen manipulation tied to COVID-19 pandemic.
In a Friday Nature Medicine publication, top U.S. health agency leaders emphasized their commitment to an executive order signed by President Donald Trump that allows for taxpayer-funded, dangerous gain-of-function (GOF) work to continue.
If GOF was the cause of the COVID pandemic that killed 1.2 million Americans, any ongoing GOF experiments represent the greatest national security risk of our time.
Leaders from the National Institutes of Health (NIH), National Institute of Allergy and Infectious Diseases (NIAID), and the Clinical Research Directorate (CRD) at Frederick National Laboratory for Cancer Research (FNLCR) will not halt GOF, but will allow it to continue under exemptions.
See the long list of never-before-seen chimeric “Frankenstein” pathogens recently created through these agencies at the bottom of this read.
In their Nature piece, NIH director Jay Bhattacharya, NIAID director Jeffery K. Taubenberger, and CRD director John H. Powers write:
“[T]he NIAID will strictly adhere to new regulatory frameworks on dangerous gain-of-function research, as defined in President Trump’s Executive Order 14292 in May 2025, and which will be established by the Office of Science and Technology Policy. We will ensure that NIH-supported research follows the new guidelines, review processes and prohibitions. Although most infectious disease research poses no catastrophic threat to human populations, those projects that do will have no part in the NIAID portfolio going forward.”
The Nature publication is behind a paywall, despite the work being funded by U.S. taxpayers.
The language of the paper gives the impression GOF work is being halted.
But Executive Order 14292, cited by the agency leaders in their Nature publication, confirms the administration is allowing GOF “exemption[s].”
Bhattacharya, Taubenberger, and Powers failed to make this clear for those who could afford access to their article.
“Heads of agencies shall report any exception to a suspension to the Director of OSTP for review in consultation with the APNSA and the heads of relevant agencies.”
This means GOF experiments are not off the table.
Michael Kratsios serves as the 13th Director of the White House Office of Science and Technology Policy (OSTP), confirmed in March 2025.
Kratsios graduated from Princeton University and interned for Senator Lindsey Graham (R-SC).
He worked in finance at Barclays Capital, Lyford Group, and as CFO of Clarium Capital, then at Thiel Capital as chief of staff to Peter Thiel.
He joined the White House in 2017 as Deputy Assistant for Technology Policy, became the fourth U.S. Chief Technology Officer in 2019, and acting Under Secretary of Defense for Research and Engineering in 2020, overseeing a $106 billion R&D budget including DARPA.
DARPA’s involvement in pandemic research predates COVID-19 and includes the agency’s rejected 2018 DEFUSE proposal to engineer novel bat coronaviruses with enhanced human infectivity, subsequent NIH-funded coronavirus manipulation, and the rapid deployment of Moderna’s mRNA platform—developed with extensive DARPA support—as the primary countermeasure once SARS-CoV-2 emerged.
Key initiatives championed by Kratsios include the American AI Initiative, National Quantum Initiative, AI regulatory principles, and international efforts like G7/G20 tech ministerials.
Post-2021, he was Managing Director at Scale AI until his 2025 OSTP return, focusing on AI, quantum, biotech, and U.S. tech leadership under President Trump.
So long as Kratsios approves the exemption, GOF work continues in the U.S.
With exemptions approved behind closed doors by a small group of political appointees, the Trump administration has yet to clearly explain where it draws the line between permissible biodefense research and experiments that could again place the United States—and the world—at catastrophic national security risk.
U.S. government is not slowing its push toward intranasal self-replicating RNA vaccine technology.
A U.S. military–funded research program has developed an intranasal, self-replicating RNA (sa-mRNA) vaccine targeting H5N1 avian influenza, built using chimeric viral constructs assembled through reverse genetics.
The work was disclosed in a 2026 Nature Communications paper and explicitly funded through a U.S. Army–administered biodefense contracting mechanism.
The vaccine is said to force cells to produce H5N1 bird flu antigen while simultaneously producing viral replication enzymes that copy the self-amplifying RNA inside the cell.
Why is the government making the bird flu pandemic problem and solution at the same time, just like it was doing with coronaviruses before the COVID-19 outbreak?
What Was Built
The researchers are said to have engineered a self-amplifying RNA vaccine that uses a Venezuelan equine encephalitis virus (VEEV) replicon backbone into which they inserted influenza hemagglutinin (HA) genes from H5N1 (and H7N9).
The RNA construct was packaged in a cationic nanostructured lipid carrier and designed for intranasal spray delivery.
This is not conventional mRNA.
Self-amplifying RNA replicates inside host cells, increasing antigen production after administration.
While the construct is described as replication-defective (it lacks viral structural genes and cannot form a spreading virus), it is nonetheless a synthetic viral system built from components of different viruses.
Reverse Genetics & Chimeric Design
The platform was produced using reverse genetics—starting from gene sequences, cloning them into plasmids, and generating RNA by in-vitro transcription.
In practical terms, this means influenza genetic material was deliberately engineered into a VEEV replicon, creating a chimeric viral construct designed to self-amplify once inside cells.
This approach represents intentional genetic assembly of viral parts to achieve a specific biological effect.
Intranasal Spray Delivery
The vaccine was purpose-built for intranasal (IN) administration, a route the authors emphasize for inducing mucosal and lung-resident immune responses that intramuscular vaccines do not generate.
The paper reports distribution throughout the upper and lower respiratory tract, with some material swallowed into the gastrointestinal tract—a confessed feature of intranasal dosing.
This delivery choice matters because it places a self-replicating RNA system directly onto respiratory mucosa, rather than confining it to muscle tissue.
The Virus Target: H5N1
The primary antigen target is H5N1 avian influenza, repeatedly framed in the paper as a pre-pandemic threat.
Ferret challenge experiments involved high-dose intranasal exposure to influenza, with the sa-mRNA platform reported to protect against severe disease.
The study positions the platform as rapidly deployable, emphasizing scalability, thermostability, and potential for stockpiling—language consistent with pandemic preparedness, not routine seasonal vaccination.
Who Funded It—& How
The paper states plainly that the work was “sponsored by the US Government under Other Transaction number W15QKN-16-9-1002.”
W15QKN-16-9-1002 is a U.S. Army Contracting Command–New Jersey Other Transaction Agreement (OTA) established under Section 815 of the 2016 National Defense Authorization Act.
The agreement created the Medical CBRN Defense Consortium (MCDC) to fund research and development of medical countermeasures for chemical, biological, radiological, and nuclear (CBRN) threats.
Key points from the OTA itself:
The agreement is administered by the U.S. Army Contracting Command on behalf of the Department of Defense.
It authorizes the government to select, direct, and fund specific projects it deems necessary.
The scope explicitly includes vaccines, medical countermeasures, and manufacturing platforms designed for rapid response to biological threats.
The estimated value of projects issued under the agreement is up to $10 billion, with a 20-year term.
The research was supported through a military biodefense R&D framework designed to develop deployable medical technologies.
Bottom Line
The Nature paper confirms that a U.S. military–administered funding program supported the development of an intranasal, spray-form self-replicating sa-mRNA vaccine built from chimeric viral constructs that include H5N1 influenza genes.
The authors emphasize speed, scalability, and deployment readiness.
This is best understood not as a routine flu-vaccine study, but as a biodefense-driven platform demonstration: a synthetic, self-amplifying viral system designed for rapid respiratory deployment in a future pandemic scenario.
At a time when governments now acknowledge that lab-engineered pathogens can spark global crises, the United States is simultaneously funding the creation of chimeric avian influenza systems and the intranasal self-replicating technologies positioned to counter them—collapsing the line between pandemic threat creation and pandemic response into the same military-run pipeline.
James Duane, a professor at Regent University School of Law, once gave a lecture with a deliberately provocative title, “Don’t Talk to the Police.” The title sounds extreme, even antisocial. It seems to counsel guilt, evasion, or hostility to lawful authority. Yet the argument Duane develops is none of these things. It is instead a sober analysis of how modern criminal procedure actually works, not how we wish it worked. When examined carefully, the conclusion he reaches is not merely defensible but compelling. Under current U.S. law, the rational course of action for any person, guilty or innocent, is to decline to answer police questions and to request a lawyer. This is not a loophole. It is the logic of the Fifth Amendment taken seriously.
Regent Law Professor James Duane gives viewers startling reasons why they should always exercise their Fifth Amendment rights when questioned by government officials.
Begin with the most basic misconception. Many people believe that talking can help them avoid arrest. They imagine that if they can just explain themselves, the officer will see their innocence and let them go. But police encounters do not begin in a neutral epistemic posture. Officers approach because they already suspect wrongdoing or because they are tasked with finding it. Their professional incentive is not to be persuaded by your narrative but to establish probable cause. This is not a moral criticism. It is a description of the job. As officers themselves openly acknowledge, a strong case is one with admissions. Confessions are not a bonus; they are the objective. Talking does not remove suspicion; it supplies material with which suspicion is formalized.
Even if arrest could theoretically be avoided through explanation, the structure of evidence law makes talking a one-way bet. Statements you make to police can almost always be used against you. Statements that help you are usually inadmissible in your favor. This is not intuitive to laypeople, but it is fundamental. Your exculpatory remarks are typically classified as your own out-of-court statements and, therefore, hearsay if you later attempt to introduce them. The prosecution, by contrast, can introduce your incriminating statements through the officer who heard them. The asymmetry is stark. Speaking hands the state admissible evidence while preserving nothing comparable for you. Silence preserves the status quo. Talking degrades it.
Consider next the case of actual guilt. Here, moral intuition often overwhelms strategic reasoning. People say one should confess for the sake of conscience or closure. But criminal law is not a sacrament. It is an adversarial system in which leverage matters. Almost all cases resolve through plea negotiations. That process is precisely where responsibility, remorse, restitution, and cooperation can be weighed in exchange for concessions. An immediate confession forfeits that leverage for nothing. Worse, even partial admissions can rescue a weak case. Evidence degrades. Witnesses disappear. Officers retire or relocate. Uncertainty is the defendant’s only bargaining chip, and confessing gives it away.
The harder and more unsettling point concerns innocence. It feels perverse to say that innocent people should fear talking more than guilty ones. Yet the data on wrongful convictions shows exactly this. A substantial portion of exonerated defendants made incriminating statements, confessed, or pled guilty. These are not abstract statistics. They reflect predictable psychological pressures. Interrogations are long. They are stressful. They exploit fatigue, confusion, and the human desire to cooperate. Suspects are fed details, assured that honesty will help, and persuaded that they are assisting in identifying the real culprit. Juries, meanwhile, treat confessions as uniquely probative. Once a confession exists, other evidence is interpreted through it. Innocence becomes an uphill argument.
Even without outright coercion, the risk of error is enormous. Perfect recall under pressure is a fantasy. Innocent people misremember times, distances, and sequences. They speak too broadly. They fill gaps. They guess. When any detail later turns out to be wrong, the narrative shifts from mistake to deception. A small inconsistency becomes evidence of consciousness of guilt. The problem is not lying. It is being human. The law, however, is unforgiving of ordinary cognitive limits when they are narrated by an officer in uniform reading from notes.
Truth itself can incriminate. This is perhaps the most philosophically important point, and it explains why the Fifth Amendment protects the innocent. You can answer every question honestly and still help complete the prosecution’s puzzle. Admitting dislike can supply motive. Describing a prior argument can establish intent. Placing yourself near a location can narrow opportunity. None of this requires falsehood. It requires only that your truthful statements be combined with other evidence you may not even know exists. The privilege against self-incrimination is not a license to lie. It is a recognition that truth can be dangerous when the state controls the narrative.
That narrative control is institutional, not personal. Police notes and testimony carry structural credibility. In court, the defendant sits beside a lawyer, already marked as someone who needs defending. The officer appears as a professional witness. When the officer recounts the defendant’s own words, recorded and framed through official notes, the story acquires an aura of objectivity. Even when no one lies, the system privileges one version over the other. Disputes about what was said rarely end in the defendant’s favor.
Talking also creates new crimes. When investigators cannot prove the underlying allegation, they often pursue charges for false statements, obstruction, or inconsistency. High-profile examples are not anomalies. They illustrate a rule. Once you speak, you are exposed to liability not only for what you did but for how accurately you recount it. Police are legally permitted to deceive during questioning. You are not permitted to be wrong. This is not an even exchange.
All of this occurs against the backdrop of an unlevel playing field by design. Modern criminal law is vast. Ordinary citizens routinely violate technical rules without knowing it. Silence is uncomfortable. People want to tell their story. Officers are trained to exploit that impulse. Time favors the state. The suspect wants to leave. The officer is content to wait. The environment is engineered to extract statements, not to neutrally discover truth.
Perhaps the most counterintuitive danger arises with alibis. A truthful alibi seems like the strongest form of exculpation. Yet if any evidence later contradicts it, even mistakenly, the alibi becomes a lie in the eyes of the jury. The prosecution gains a powerful narrative of deception layered on top of the original charge. What would have been a thin case becomes a compelling one, built largely from the defendant’s own words.
The conclusion follows with uncomfortable clarity. Speaking to police is volunteering to play an away game under rules you did not write and cannot change. Your helpful statements are unlikely to help you later. Your harmful statements can be used immediately. Your memory will be imperfect. The officer’s notes will be authoritative. Even truth can be weaponized. The rational response is not defiance but restraint.
Identify yourself if required by law. Then say you are invoking your right to remain silent and that you want a lawyer. Then stop talking. This advice is not cynical. It is constitutional realism. The Fifth Amendment is not an admission of guilt. It is an acknowledgment of how power, incentives, and human cognition actually operate. Taking it seriously means using it or facing the ugly consequences of ignoring it and not putting it into practice. Period. End of story. Full stop already. You have preciously been warned.
New records show top U.S. nuclear, national security laboratories scrutinized primers used to define the pandemic—but hid the results.
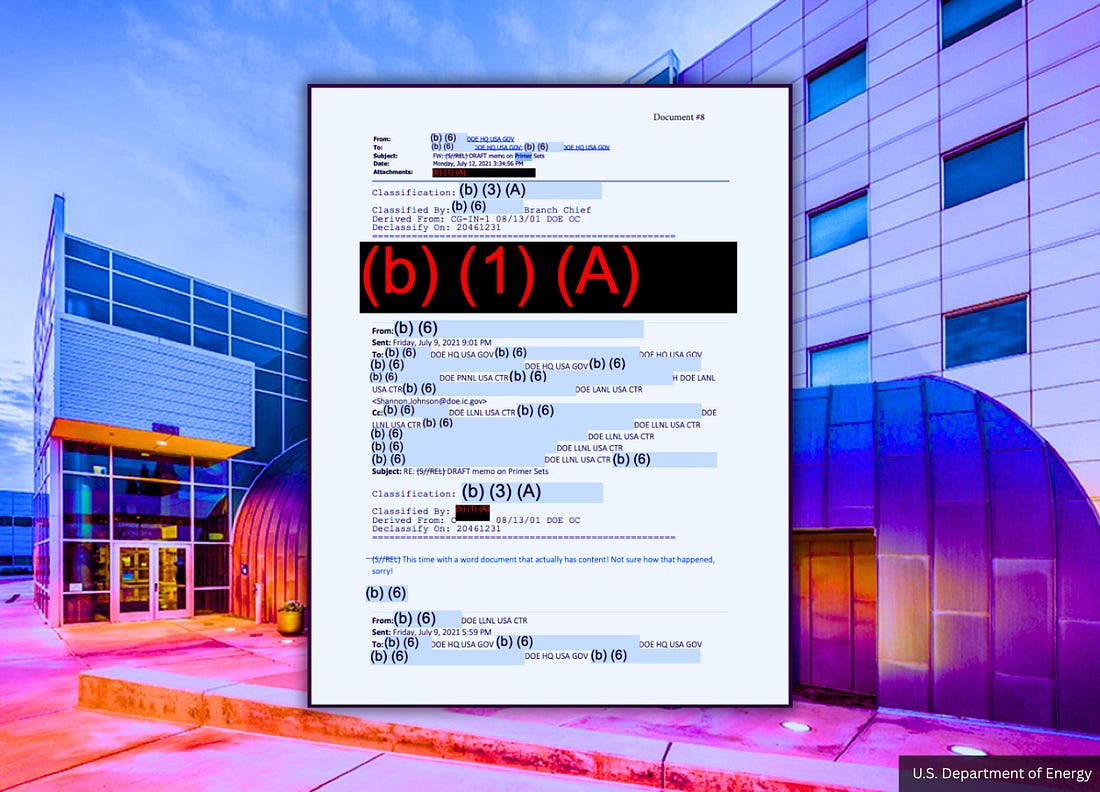
Newly released Department of Energy (DOE) records obtained by U.S. Right to Know through a Freedom of Information Act (FOIA) requenst show that U.S. federal intelligence agencies classified and redacted the results of an internal review of COVID-19 PCR test primers, even as those tests were used to define “cases,” drive emergency policy, and justify unprecedented social and economic controls.
The documents reveal that during the pandemic, the U.S. government quietly subjected PCR test primer sets—the molecular components that determine what PCR tests detect—to classified scrutiny by top national security laboratories, while withholding the findings from the public under national-security and intelligence exemptions.
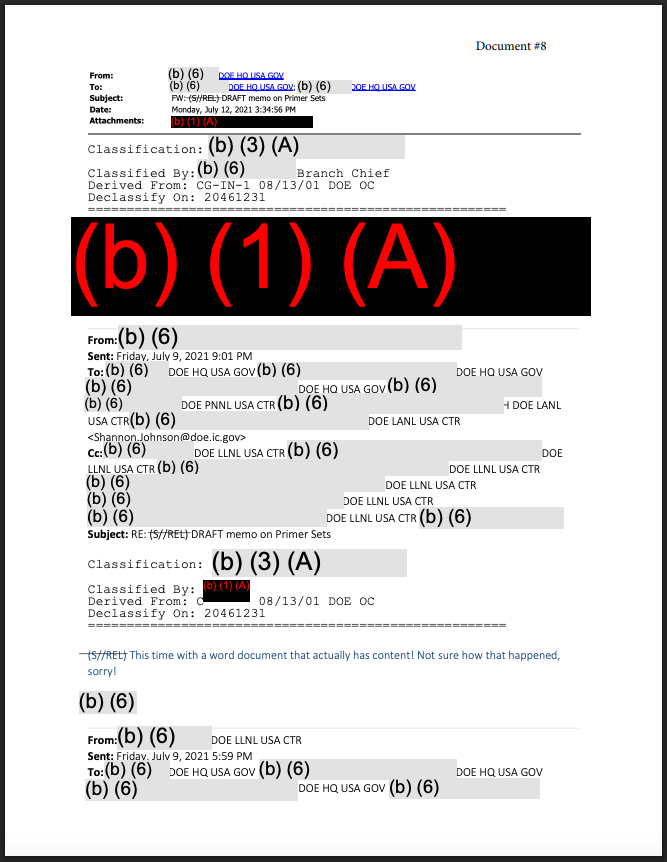
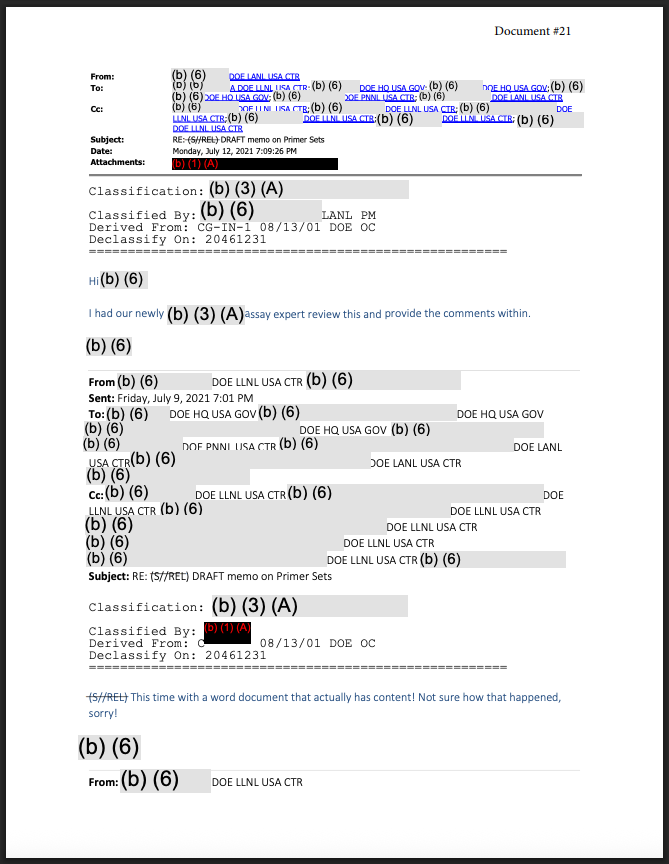
At the center of the release is a classified internal communication titled “DRAFT memo on Primer Sets,” circulated through the DOE’s Office of Intelligence and Counterintelligence and reviewed by assay experts at Lawrence Livermore National Laboratory, Los Alamos National Laboratory, and Pacific Northwest National Laboratory.
The memo itself remains classified.
Its conclusions were redacted.
No public explanation was ever provided.
PCR Testing Was Treated as a Classified Intelligence Issue
PCR tests do not detect an intact virus and do not prove infection.
They work by using short genetic sequences—primers—to bind to matching genetic material and amplify it until a signal is detected.
What a PCR test detects depends entirely on what its primers bind to.
The DOE records show that this foundational question—what COVID-19 PCR tests were actually detecting—was handled not as a public scientific matter, but as a classified intelligence issue.
One internal email chain explicitly references a classified document titled:
“FW: (S//REL) DRAFT memo on Primer Sets”
Another message states that the memo was reviewed by a specialist:
“I had our newly assay expert review this and provide the comments within.”
The routing shows coordination across DOE intelligence offices and U.S. national security laboratories.
The content of the memo, the concerns it addressed, and the conclusions it reached are all withheld from public release.
What the Government Did Not Disclose
Throughout the pandemic, the public was repeatedly told that COVID-19 PCR testing was reliable, specific, and settled.
Questions about PCR design were often dismissed as misinformation.
The DOE records show the opposite posture inside government: PCR primer design was serious enough to warrant classified review by nuclear-era national laboratories, with the results deemed sensitive enough to be redacted under national-security and intelligence-source protections.
DOE explicitly justified withholding the information by citing risks to national security and intelligence methods, and assigned declassification dates decades into the future.
There is no indication in the records that the findings were shared with public-health agencies, published in scientific journals, or communicated to the public.
Why PCR Primer Design Is Existential, Not Technical
PCR testing formed the backbone of the pandemic response.
PCR “positives” were treated as synonymous with infection and were used to define:
COVID “cases”
Community spread
Hospital surges
Lockdowns and emergency orders
Vaccine emergency authorizations
If PCR primers bind to viral genetic material, positives reflect virus detection.
If PCR primers bind to human genetic material, positives can reflect the person being tested.
That distinction determines whether a “case” is an infection—or merely a genetic detection.
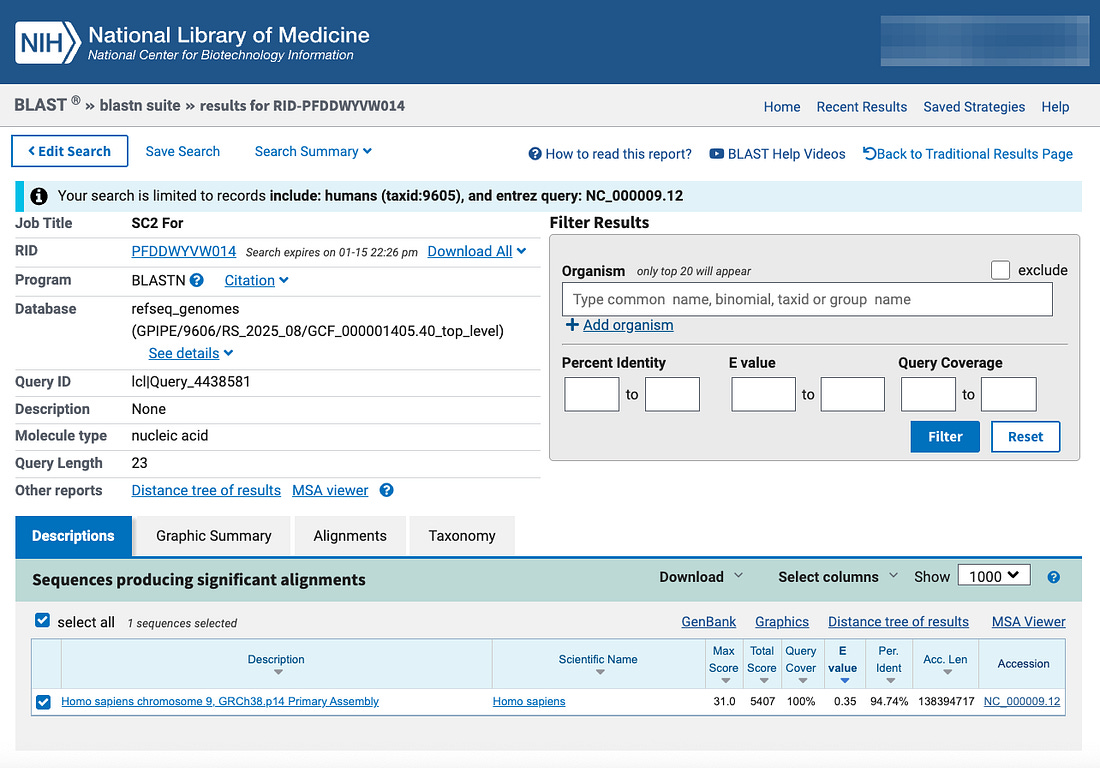
The results show that the primer has multiple perfect and near-perfect matches to the human genome, including:
Repeated 13–16 base stretches with 100% identity to human DNA
Longer alignments exceeding 94–95% identity across multiple human chromosomes
In plain terms: the CDC’s COVID-19 PCR primer can bind to human genetic material.
That establishes a biological mechanism by which a PCR test administered “for COVID-19” can return a positive result by amplifying human DNA or RNA rather than viral RNA.
If that occurs, the test still produces a positive signal.
The result is still recorded as a “COVID case.”
But no infection has been detected.
The “case” is a human genetic detection.
Why This Explains the Secrecy
The DOE records show that this was not ignored.
It was escalated—and then classified.
National security laboratories are not tasked with reviewing PCR primer sets unless the implications are systemic.
If the test used to define a global pandemic can generate positives without detecting a virus, public disclosure would collapse the legitimacy of case counts, emergency powers, and pandemic policy itself.
The records show that U.S. intelligence examined the issue.
They also show that the findings were classified, redacted, and withheld from the public.
The United States accepted a digital genetic code supplied by the Chinese government—without access to the physical lung sample it was allegedly sequenced from—and relied on PCR testing and that same in-silico sequence to define cases, drive emergency policy, and later encode spike protein into hundreds of millions of vaccine doses.
That secrecy is even more consequential given that U.S. military planners had already built—and quietly funded—a DARPA-backed pandemic pipeline designed to treat digital genetic sequences as functional viruses, synthesizing infectious clones and mass-producing mRNA countermeasures without requiring a verified physical pathogen, meaning both COVID “case” detection and the subsequent vaccine rollout rested on the same unverified, in-silico genetic foundation.
Dr. Kary Mullis, the late inventor of the PCR test, said in a 1997 interview (here) that his test should not be used to determine whether a subject is infected with a virus.
This is because the test “can find almost anything in anybody” if its parameters are set high enough, tainting the results, according to the Nobel Prize winner.
“Anyone can test positive for practically anything with a PCR test. If you run it long enough… you can find almost anything in anybody,” Dr. Mullis said. “It doesn’t tell you that you’re sick.”
Mullis’s warning matters because it confirms that PCR was not designed to establish clinical infection, meaning a pandemic built on PCR “cases” can reflect amplified genetic signals rather than illness—a vulnerability that could be serious enough to later draw classified scrutiny from U.S. national security laboratories.
What the Records Prove—& What They Imply
The documents do not release the primer memo.
They do not disclose the conclusions.
They do not quantify how many PCR positives may reflect human material.
They do prove that:
COVID-19 PCR test primers were scrutinized by U.S. intelligence
Top national security laboratories were involved
The findings were classified and redacted
The public was never informed
Combined with sequence-alignment evidence showing that the CDC’s PCR primer binds to human DNA, the implication is unavoidable:
The U.S. government privately examined whether the test used to define the pandemic could generate “cases” without detecting infection—and then classified the answer.
The DOE records were released to U.S. Right to Know under FOIA request HQ-2025-03244-F.
The primer alignment is reproducible using the CDC’s published primer sequence and the human reference genome.
The public was told PCR testing was settled science.
The documents show the government didn’t treat it that way behind the scenes.
And whatever they found, they made sure we were never allowed to see it.



















Recent Comments