
Massachusetts Advances H5N1 Influenza Bird Flu Bill with Quarantine Protocols, Surveillance Grid, and Vaccination Strategies
Lawmakers move avian influenza response infrastructure into study pipeline while preserving full operational framework.

A Massachusetts bill laying out a full-scale response system for H5N1 avian influenza “bird flu” is advancing through the legislature—constructing quarantine protocols, mass surveillance systems, vaccine deployment planning, and statewide clinical trial infrastructure around a single named virus before any declared widespread outbreak.
The move comes as state, federal, and international actors are orchestrating the systems, infrastructure, and response mechanisms surrounding a future bird flu pandemic.
Massachusetts House Bill 2385 (H2385), introduced February 27, 2025 by Representative Leigh Davis (D-3rd Berkshire), does not address general pandemic preparedness.
Instead, it is specifically targeted at H5N1 bird flu, directing the state to build a coordinated response system spanning human, livestock, and wildlife populations under a single-disease framework.
On March 16, 2026, lawmakers moved the bill into a Public Health study order (H5234), advancing the proposal into a formal development phase—preserving the full framework while removing it from an immediate vote.
After sitting untouched for over a year, the bill was suddenly acted on and moved into a study process—signaling it had become important enough to preserve and develop, but not yet ready to pass in its current form.
You can contact Rep. Davis’ office here and the rest of the Massachusetts representatives here to voice your opinion on the bill.

Emergency Bird Flu Powers Activated Up Front
The bill opens with emergency language:
“declared to be an emergency law, necessary for the immediate preservation of the public health.”
This positions the H5N1 response system for rapid activation, not gradual implementation.
Mass Bird Flu Surveillance Across Humans & Animals
The bill directs:
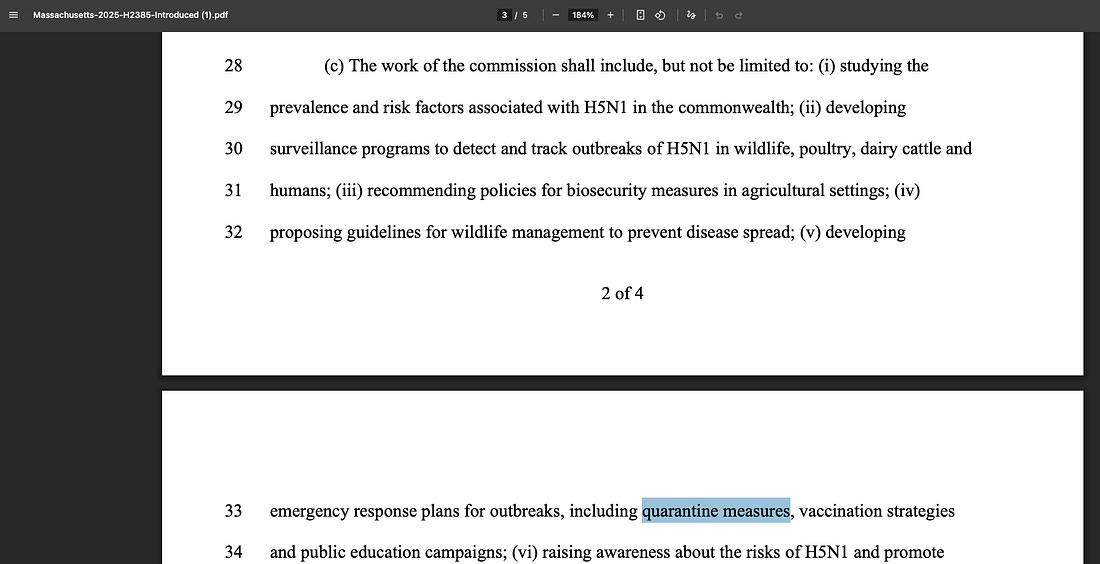
“developing surveillance programs to detect and track outbreaks of H5N1 in wildlife, poultry, dairy cattle and humans”
This creates a multi-species surveillance system focused specifically on bird flu, linking:
- agricultural environments
- wildlife reservoirs
- human cases
into a centralized tracking network.
Quarantine & Vaccine Plans Pre-Built for H5N1
The commission is tasked with designing:
“emergency response plans… including quarantine measures, vaccination strategies”
This establishes predefined intervention mechanisms, including:
- quarantine and isolation protocols
- movement restrictions tied to exposure
- coordinated vaccine deployment strategies
—all built specifically around bird flu response.
Statewide Bird Flu Trials Ready for Rapid Deployment
The bill calls for:
“preparation to launch statewide clinical trials that swiftly evaluate… novel therapeutic approaches”
This enables:
- rapid testing of treatments during an H5N1 event
- deployment of experimental or emerging interventions
- statewide scaling of trials
Farm Testing Network Expands Bird Flu Detection
The legislation includes:
“production of self-administered swabs… distributed to farms… allowing workers to… screen themselves”
This creates a continuous testing system tied directly to bird flu monitoring in:
- farms
- livestock environments
- worker populations
Drug Stockpiles Expand as Bird Flu Mutation Expected
The bill directs:
“shoring up of stockpiles… beyond Tamiflu… guard against viruses mutating”
This anticipates:
- mutation of H5N1
- purported need for expanded pharmaceutical reserves
- long-term treatment preparedness tied to bird flu
Private Funding Flows Into Bird Flu Response System
The commission is authorized to receive:
“funds from public and private sources such as gifts, grants and donations.”
This integrates:
- private funding sources
- external organizations
- non-government actors
into state bird flu response infrastructure.
Centralized Control System Coordinates Bird Flu Response
The bill mandates:
“coordinating efforts among government agencies… public health entities”
This establishes a centralized response model specifically for bird flu, aligning:
- public health agencies
- agriculture
- research institutions
Bill Quietly Advanced Into Study Pipeline Without Vote
The proposal remains active:
- Folded into study order H5234
- Discharged from Public Health Committee
- Transferred to the House Rules Committee
This keeps the full H5N1-focused framework moving through the legislative pipeline, positioning it for future action.
Bottom Line
H2385 is not a general preparedness bill.
It builds a targeted operational framework around avian influenza (H5N1) specifically.
The bill establishes:
- A bird flu surveillance grid across humans, livestock, and wildlife
- Predefined quarantine and vaccination protocols tied to H5N1
- A statewide clinical trial system ready for deployment
- A continuous testing pipeline in agricultural settings
- Expanded drug stockpiling anticipating mutation
- A public-private funding structure embedded in response planning
- A centralized command system for coordinated bird flu response
Lawmakers have now moved this framework into a formal study process—keeping it active and positioning it for future rollout.



















Recent Comments