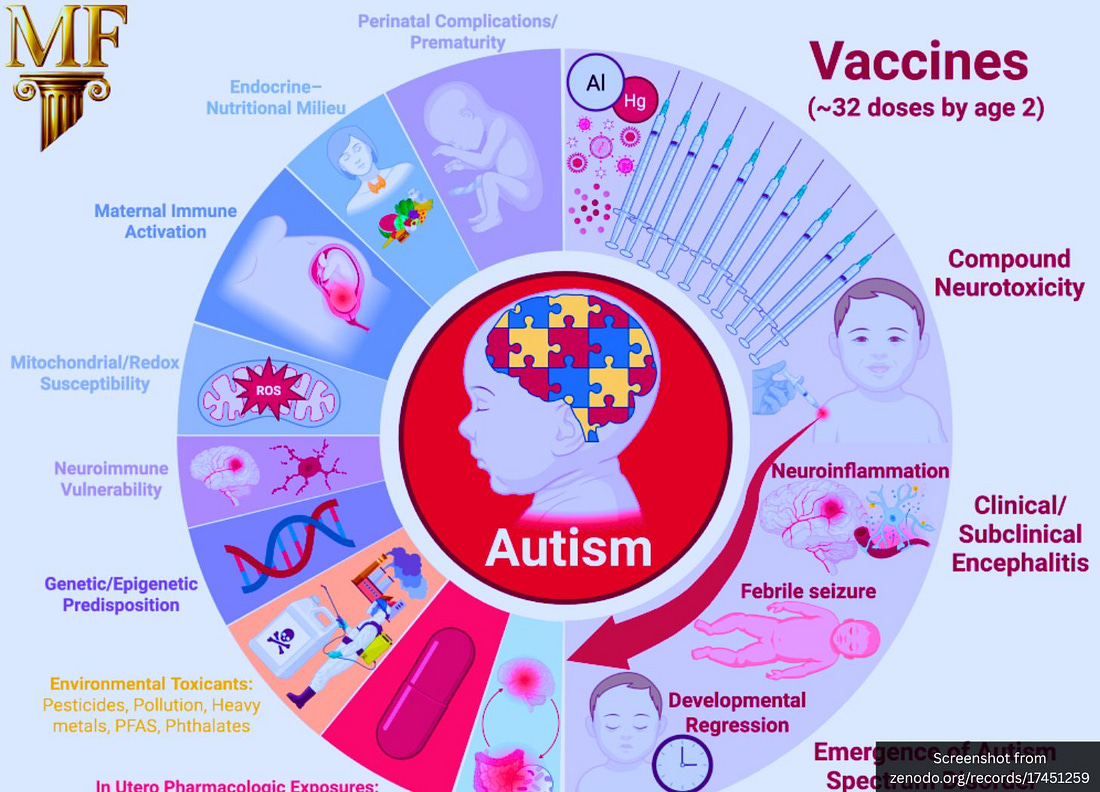
“Childhood vaccination constitutes the most significant modifiable risk factor” for autism, write Hulscher, McCullough, Wakefield, and seven other researchers.
A sweeping new analysis by the McCullough Foundation has confirmed that “the most significant modifiable risk factor” for autism is childhood vaccination.
The majority of them suggest the current vaccine schedule represents an “urgent public health priority” regarding autism.
That means vaccines—with a market value estimated at $82 billion in 2025 and expected to reach $125 billion worldwide by 2032—are likely causing one of the most devastating and tragic disorders known to mankind.
The authors write:
“Combination and early-timed routine childhood vaccination constitutes the most significant modifiable risk factor for ASD, supported by convergent mechanistic, clinical, and epidemiologic findings, and characterized by intensified use, the clustering of multiple doses during critical neurodevelopmental windows, and the lack of research on the cumulative safety of the full pediatric schedule. As ASD prevalence continues to rise at an unprecedented pace, clarifying the risks associated with cumulative vaccine dosing and timing remains an urgent public health priority.”
Most Studies Indicate a Vaccine Association
The McCullough Foundation examined more than a hundred publications that evaluated links between vaccination and neurodevelopmental outcomes.
Most of them pointed to vaccines being the problem.
The authors write:
“Of 136 studies examining childhood vaccines or their excipients, 29 found neutral risks or no association, while 107 inferred a possible link between immunization or vaccine components and ASD or other neurodevelopmental disorders (NDDs).”
In other words, nearly four out of five studies reviewed showed some level of correlation between vaccine exposure and neurodevelopmental changes.
No Long-Term Study of the Full Vaccine Schedule Exists
The report reveals that safety testing has never evaluated the cumulative vaccine program that children actually receive.
“To date, no study has evaluated the safety of the entire cumulative pediatric vaccine schedule for neurodevelopmental outcomes through age 9 or 18 years. Nearly all existing research has focused on a narrow subset of individual vaccines or components—primarily MMR, thimerosal-containing, or aluminum-adjuvanted products—meaning that only a small fraction of total childhood vaccine exposure has ever been assessed for associations with ASD or other NDDs.”
Each vaccine is licensed individually, but children are exposed to dozens in combination.
This is a major regulatory gap that undermines every “safe and effective” claim made about the schedule as a whole.
Unvaccinated Children Reported to Have Better Overall Health
The authors highlight a subset of comparisons between vaccinated and completely unvaccinated populations.
“Twelve studies comparing routinely immunized versus completely unvaccinated children or young adults consistently demonstrated superior overall health outcomes among the unvaccinated, including significantly lower risks of chronic medical problems and neuropsychiatric disorders such as ASD.”
These findings show a reproducible pattern across independent datasets.
That suggests vaccine exposure correlates with poorer long-term health outcomes.
Authors Argue Vaccine Ingredients Can Damage the Brain
The report analyzes the biological plausibility of vaccine-related neuroinflammation.
“Antigen, preservative, and adjuvant (ethyl mercury and aluminum) induced mitochondrial and neuroimmune dysfunction, central nervous system injury, and resultant incipient phenotypic expression of ASD.”
They describe a cascade in which aluminum and mercury trigger oxidative stress and mitochondrial injury in susceptible children.
This is offered as the mechanistic foundation for their broader argument.
Timing and Clustering of Shots Said to Heighten Risk
The authors also show that timing is critical—that multiple shots at once magnify danger.
“Clustered vaccine dosing and earlier timing of exposure during critical neurodevelopmental windows appeared to increase the risk of ASD.”
They argue that vaccine-induced immune stimulation during rapid brain growth in childhood can lead to chronic inflammation.
The paper draws attention to the timing between federal liability protection for manufacturers and rising autism rates.
“The most salient feature of this steeply rising trend of autism incidence and prevalence is that it began shortly after the passage of the National Childhood Vaccine Injury Act (NCVIA) in 1986… Since then, the number of new vaccines on the childhood schedule has greatly proliferated from 12 shots in 1986 to 54 shots in 2019.”
The authors link legal immunity for manufacturers to rapid schedule growth.
This is evidence that financial and regulatory incentives expanded exposure while suppressing safety accountability.
Bottom Line
The McCullough Foundation report lays out multiple powerful arguments that challenge decades of public-health assurances:
most reviewed studies show a possible link;
unvaccinated children fare better;
cumulative schedule testing is absent;
vaccine ingredients and timing may trigger neuroinflammation;
and the surge in autism parallels expansion of the vaccine schedule.
The report’s scale and the reputations of its authors ensure its arguments will expose the significant dangers posed by vaccines.
If even part of what the report alleges is accurate, it suggests that modern public health policy has neglected the most consequential safety question of our time: What happens when the cumulative biological burden of vaccination collides with the developing human brain?
Thousands of BSL-3 labs worldwide now handle pathogens like bird flu, SARS-CoV-2, and tuberculosis—with almost “no oversight,” biosecurity experts confirm.
Over the past few years, the world has entered a new era of high-containment biological research—marked by a dramatic expansion of laboratories capable of working with the most lethal viruses known to man.
These include facilities built to the highest biosafety standard, Biosafety Level 4 (BSL-4), and they carry not only the broken promise of defending us from pandemics but also the danger of enabling bioweapons creation, whether by accident or deliberate misuse.
Strikingly, a May 2025 Journal of Public Healthstudy found that more than 90% of the countries with at least one BSL-3 laboratory lacked oversight or regulation of dual-use research of concern.
Dual-use research refers to experiments that can be used for good (e.g., alleged drug development) but also for harm (e.g., creating a bioweapon).
The Journal of Public Health study aimed to investigate the worldwide distribution of BSL-3 and BSL-4 laboratories.
Alarmingly, it found that:
“No international organization has a comprehensive register or global oversight of Biosafety Level 3 (BSL-3)/BSL-4 laboratories. Different countries use different standards for designation of pathogens and laboratories.”
“More than 90% of the countries with at least one BSL3 laboratory have no oversight/regulations regarding dual-use research.”
BSL-3 laboratories work with serious or potentially lethal pathogens that can be transmitted through the air and usually have available treatments or preventions, such as tuberculosis, SARS-CoV-2 (COVID), and avian influenza “bird flu.”
BSL-4 laboratories handle the most dangerous and exotic pathogens that often cause fatal diseases with no available vaccines or treatments, such as Ebola and Marburg viruses.
Taken together, the proliferation of BSL-3 and BSL-4 labs around the world raises national security, informed consent, and conflict of interest concerns.
They raise national security concerns because accidental or intentional lab leaks put American lives at risk, clearly proven by the COVID-19 pandemic. Congress, the White House, the Department of Energy, the FBI, and the CIA have confirmed that the COVID pandemic was likely the result of lab-engineered pathogen manipulation.
They raise informed consent concerns because citizens are often unknowingly and/or unwillingly exposed to risks from nearby labs or experimental pathogen releases conducted without public awareness or approval.
They raise conflict of interest concerns because many of these labs are funded by entities that profit from the development of pathogens and drugs that target those pathogens, meaning they benefit financially from an accidental or intentional lab leak-caused outbreak.
Even former NIAID Director Anthony Fauci—who dismissed claims that a lab leak caused the COVID pandemic—has admitted in print that the greatest biosecurity threat regarding dangerous pathogen research is laboratory “insiders who have direct access” to the pathogens or “outsiders who collaborate with or subvert insiders.”
Given the mounting evidence of accidents, secrecy, and conflicts of interest, the continued operation of these bioweapons labs poses an unacceptable threat to humanity’s safety.
The only responsible course is to shut down all BSL-4 facilities worldwide and impose a global moratorium on high-risk pathogen experiments in order to prevent further catastrophe.
But governments all over the world are doing the opposite.
The Journal of Public Health authors warn in their conclusion:
“The number of BSL-3 and BSL-4 laboratories is continually increasing, and many do not have adequate biosafety guidelines.”
Dr. Richard Bartlett warned that COVID-19 resulted from dangerous lab experiments and urged a global ban on bioweapons, calling the unchecked spread of BSL-3 and BSL-4 labs—where such pathogens are made—an existential threat to humanity.
“President Trump recently spoke to the UN General Assembly, stating that COVID was the result of risky laboratory experiments and that the United States would lead an effort to ban bioweapons,” he told this website.
“The White House, U.S. Congress, FBI, CIA, German intelligence, and the Department of Energy’s intelligence division have all acknowledged that COVID ‘may have’ originated from a lab. Bioweapons are developed in BSL-3 and BSL-4 laboratories. Yet no one has been held accountable for the worst catastrophe in U.S. history. The continued proliferation of BSL-3 and BSL-4 labs worldwide shows that we have learned nothing from this disaster. Bioweapons, like nuclear weapons, are weapons of mass destruction—and the stockpiling of pathogens such as avian flu represents an existential threat to humanity.”
Worldwide Surge of Bioweapons Labs
Before the COVID pandemic, only a modest number of BSL-4 labs existed worldwide.
Mapping studies published earlier this year show there are now more than 100 operational BSL-4 labs across 34 countries.
Researchers identified a staggering 3,515 BSL-3 laboratories in 149 countries.
They write in their Journal of Public Health publication:
“We identified 3,515 BSL-3 laboratories in 149 countries, with nearly half (47.1%) in the United States. Details on geolocations and pathogens they handled are publicly available for 955 of these labs. The United Kingdom had the highest rate (N = 9) of BSL-3 labs per million population, while Bangladesh had the lowest. High-income countries house 82% of these laboratories. There are 110 BSL-4 laboratories in 34 middle- and high-income countries, and 46% are in the WHO’s Europe region. Notably, from the health security index perspective, 91.6% of countries with at least one BSL-3 laboratory lack guidelines for dual-use research of concern.”
India’s Ambitious Expansion
In India, the Defence Research & Development Establishment (DRDE) in Gwalior inaugurated a BSL-4 facility in November 2024, aimed at experimenting with Nipah virus and Crimean‑Congo hemorrhagic fever virus.
Additional high-containment labs are planned, potentially creating one of Asia’s largest BSL-4 networks.
Russia’s flagship BSL-4 facility at State Research Center of Virology and Biotechnology VECTOR (Koltsovo) is already a key part of its bio-infrastructure.
Under the national “Sanitary Shield” program, Moscow announced plans for up to 15 new “maximum-biosafety level” labs by 2024.
While not all details are public, satellite imagery and defense analysis suggest that several facilities—such as the site at Sergiev Posad‑6 near Moscow—exhibit features consistent with BSL-4 design.
United States: Updating an Already Extensive Network
The United States remains home to one of the largest portfolios of BSL-4 labs globally, with around 14 active facilities as of 2023.
These include institutions such as the Galveston National Laboratory, Boston University National Emerging Infectious Diseases Laboratories (NEIDL) and others managed by the Centers for Disease Control and Prevention (CDC).
Construction is underway for a new state-of-the-art BSL-4 laboratory at the CDC’s Roybal campus in Atlanta, Georgia, as part of the CDC’s 2025 Masterplan.
The new facility, called the High Containment Continuity Laboratory (HCCL), will be a 160,000-square-foot, multi-story research building designed to accommodate approximately 80 laboratory researchers.
Latin America’s Entry: Brazil & Argentina
In Brazil, the Brazilian Center for Research in Energy and Materials (CNPEM) broke ground in 2024 on a proposed BSL-4 complex dubbed “Orion,” to be integrated with the country’s Sirius synchrotron light-source.
If realized, it would become South America’s most advanced high-containment biology facility.
In Argentina this month, the Malbrán Institute in Buenos Aires opened the country’s first BSL-4 lab.
As an international hub for migratory birds traveling between the Northern and Southern Hemispheres, Argentina’s position makes it a strategic focal point in the global network of avian flu surveillance and experimentation—placing it squarely within the larger international orchestration of a potential bird flu pandemic currently underway.
Bottom Line
The global explosion of BSL-4 laboratories represents not progress, but peril.
What governments call “pandemic preparedness” has become an uncontrolled arms race in bioweapon capability, with more than 110 BSL-4 labs now operating across 34 countries—most in nations that have no enforceable oversight of dual-use research.
The same systems meant to prevent pandemics are engineering the conditions that could ignite the next one.
With over 90% of countries hosting BSL-3 labs lacking any regulation of dual-use research, humanity is effectively constructing a worldwide bioweapons network under the banner of science.
These facilities have already demonstrated fatal lapses, secrecy, and conflicts of interest—and the agencies that fund them often profit from both the creation of pathogens and the “solutions” they sell afterward.
Given this reality, nothing short of a global moratorium on high-risk pathogen research and the immediate closure of all BSL-4 laboratories can protect public safety.
The question is no longer if another lab-engineered outbreak will occur, but how many more chances we are willing to give it to happen again.
Back-to-back 2025 summits in Melbourne unite the world’s leading influenza and pandemic-therapeutics researchers—while nations engineer bird-flu viruses and vaccines in parallel.
Australia’s Peter Doherty Institute for Infection and Immunity will host two international summits over six weeks that together represent an unprecedented coordination of global pandemic planning—one devoted to “next-generation therapeutics,” the other to influenza viruses, which include H5N1 bird flu.
Both come as laboratories worldwide create never-before-seen avian-influenza bird flu strains and test the vaccines that would be forced on populations in the event of a potential outbreak or an accidental—or intentional—laboratory leak.
October 27: “Next-Generation Therapeutics for Pandemic Preparedness.” Hosted by the Cumming Global Centre for Pandemic Therapeutics, a 20-year, $250 million initiative based at the Doherty Institute, the panel will bring together Professor Sharon Lewin (Doherty Institute), Professor David Ho (Columbia University), Professor Linfa Wang (Duke-NUS Singapore), and Professor Nanshan Zhong (Guangzhou National Laboratory). The discussion will be moderated by New York Times science journalist Apoorva Mandavilli.
November 13–14: 16th Australian Influenza Symposium. Organized by the WHO Collaborating Centre for Reference and Research on Influenza, also housed at the Doherty Institute, the symposium will focus on influenza viruses—which include H5N1 “bird flu,” COVID-19, and RSV—with speakers from the United States, United Kingdom, Hong Kong, and Cambodia.
Together, these back-to-back meetings merge pandemic preparedness, vaccine platform innovation, and influenza virology into one integrated agenda—precisely as governments worldwide invest billions into bird-flu gain-of-function research and vaccine manufacturing pipelines.
This unprecedented domestic investment followed the United States’ own 1$ billion allocation for a future influenza pandemic in its March 2024 omnibus spending bill—together forming a synchronized, pre-outbreak global financing network for bird-flu research, response, and vaccine development.
That synchronized U.S. funding drive has since deepened: in May 2025, the Trump Administration launched a $500 million “Generation Gold Standard” initiative through HHS and NIH to develop so-called “universal” pandemic vaccines—focusing primarily on H5N1 avian influenza, the same virus U.S.-funded gain-of-function experiments have been enhancing in laboratories.
International ‘Problem-Solution’ Pattern
The emerging pattern is unmistakable: governments and research institutions around the world are simultaneously engineering more dangerous strains of avian influenza while developing lucrative vaccines and therapeutics to counter those very same lab-made threats.
Just like they did before the COVID-19 pandemic.
1. The ‘Problem’: Engineered Bird Flu Pathogens
International state-funded researchers have deliberately created or enhanced H5N1 and related influenza viruses under the banner of “pandemic preparedness.”
United States (CDC, Georgia): A npj Viruses study revealed that the Centers for Disease Control and Prevention (CDC) engineered a new H5N1 bird flu strain with enhanced immune system evasion, suppressing host interferon signaling to make the virus harder to detect and more transmissible.
United States (USDA, NIH, NIAID, Nebraska): A separate U.S. Department of Agriculture study, backed by NIH and NIAID, confirmed the creation of lab-engineered bird flu viruses with enhanced replication and growth traits, conducted in Nebraska under high-containment conditions.
United States & South Korea (Joint Project, Georgia): In a Virology journal paper, U.S. and South Korean scientists collaborated to create “Frankenstein” bird flu viruses, merging multiple influenza strains through reassortment and gain-of-function modification—explicitly designed to assess pandemic potential.
China (Two H5N1 Constructs): Chinese researchers created two novel H5N1 constructs, one with 64× stronger binding affinity to host cells, and another 100% lethal in mammal models—both representing extreme gain-of-function outcomes justified as “host adaptation” studies.
United Kingdom (Neurological & Transmission Gains): In the Journal of General Virology, British scientists engineered two new bird flu viruses that produced neurological symptoms and enhanced transmission efficiency, directly modifying viral genes tied to host tropism and central nervous system infection.
Together, these projects represent a coordinated global escalation of avian influenza manipulation, where government-backed labs on multiple continents are simultaneously designing new, more dangerous viral genotypes under the guise of “prevention.”
2. The ‘Solution’: Vaccines & Pharmaceutical Countermeasures
At the same time, governments and their industry partners are fast-tracking bird flu countermeasure programs worth hundreds of millions of dollars, creating a mirror image to the COVID-19 playbook.
United States (HHS/BARDA–Cidara Collaboration): This month, the Biomedical Advanced Research and Development Authority (BARDA) awarded Cidara Therapeutics $339 million to advance its injectable influenza drug CD388, designed to treat and prevent pandemic influenza. The funding explicitly supports domestic manufacturing and supply-chain readiness—before any outbreak occurs.
Russia (Vector Institute): Meanwhile, the Vector Institute developed a lab-made bird flu spike protein formulated for needle-free jet injection, as published in Vaccines. This “next-generation” countermeasure mimics Western self-amplifying vaccine research and shows that both East and West are preparing pharmacological solutions to the same engineered viral problem.
3. Coordinated Crisis Creation
This dual track—create the pathogen, then sell the cure—echoes the pattern seen before COVID-19, when EcoHealth Alliance’s DEFUSE project proposed engineering chimeric coronavirus spikes and aerosolized self-spreading vaccines years before the 2019 outbreak.
A Frontiers in Virology study later confirmed that Moderna’s 2016 patented spike protein sequence—developed years before the COVID-19 outbreak—matched the pandemic virus’s spike sequence with a one-in-three-trillion probability of occurring naturally, underscoring how the vaccine blueprint pre-dated the very pathogen it was said to counter.
Subsequent congressional findings revealed that DARPA, the Department of Defense, and the Office of the Director of National Intelligence had classified and concealed EcoHealth Alliance’s DEFUSE proposal—the very plan that outlined how to engineer SARS-like viruses with furin cleavage sites—prompting Senator Roger Marshall to warn the cover-up may “rise to the level of misconduct, false statements, obstruction of federal proceedings, conspiracy, conflicts of interest, or infractions of administrative or civil laws.”
With the CDC, USDA, NIH, and foreign counterparts now constructing novel bird flu strains while multinational vaccine platforms and contracts proliferate in parallel, and with the very same agencies that concealed the COVID-19 gain-of-function blueprint now leading global influenza programs, the question that must be asked is no longer if governments are orchestrating a coordinated bird flu “response,” but how far in advance that response was planned.
A Global Replay Under a New Virus
The DEFUSE model of pathogen engineering paired with vaccine development has simply migrated from coronaviruses to influenza viruses.
The Doherty Institute’s consecutive summits reflect that shift, serving as a coordination hub for the same kind of pre-outbreak collaboration that characterized the years leading up to 2020.
Already, governments have:
Pledged billions in pre-emptive pandemic funding,
Approved dual-use bird-flu experiments, and
Established emergency vaccine frameworks identical to those used for COVID-19.
And once again, the institutions creating the potential pandemic are the same ones designing and licensing the vaccines that will follow.
Doherty’s summits are reminiscent of an event that was held in New York just weeks before the COVID pandemic hit.
That event, called Event 201, was a pandemic simulation exercise conducted on October 18, 2019, in New York City.
It was jointly hosted by the Johns Hopkins Center for Health Security, the World Economic Forum (WEF), and The Bill & Melinda Gates Foundation.
The COVID pandemic would commence that December, compelling many to point to Event 201 as evidence that global parties had orchestrated the COVID pandemic.
Historical Pattern: Experimentation Without Consent
Public skepticism toward “preparedness” programs is grounded in undeniable history.
Tuskegee Syphilis Study (1932–1972): The U.S. Public Health Service deliberately withheld treatment to study disease progression.
Operation Sea-Spray (1950): The U.S. Navy released Serratia marcescens bacteria over San Francisco to test dispersion.
Operation Big City (1956) and Operation Large Area Coverage (1957–58): The U.S. Army dispersed zinc cadmium sulfide particles over major American cities.
All were officially justified as “defensive research.”
All were later admitted.
That record raises the inescapable question: if governments have repeatedly conducted biological experiments on civilians without consent, why should current “preparedness” programs be accepted at face value?
The Unprecedented Nature of the Doherty Coordination
What makes the October and November 2025 Doherty summits different is the scale and precision of international coordination—the first time pandemic-therapeutic and influenza-pathogen leaders will gather under one roof at a moment of simultaneous H5N1 experimentation across the world.
Australia’s own billion-dollar bird-flu program, America’s parallel funding, and WHO’s new Pandemic Agreement all converge here, turning Melbourne into a symbolic and literal meeting point for the next global bioresponse architecture.
Are these events truly about preparedness—or are they the next chapter in an orchestrated cycle where the same governments and corporations create both the outbreak and the opportunity?
Bottom Line
The Doherty Institute is now hosting one of the most consequential pandemic coordination meetings since COVID-19—and they arrive at the exact moment governments are engineering, testing, and vaccinating against new H5N1 strains.
The COVID precedent is clear: before the pandemic, scientists developed the spike sequence and vaccine technology that later matched the outbreak virus itself—with the same institutions funding both the research and the remedy.
Today, as H5N1 undergoes genetic manipulation across continents and billions flow into vaccine development before any outbreak, the pattern is unmistakable.
And ask yourself, and Secretary Kennedy, why he’s approving more and more of them. Safe for whom? Effective at what?
On September 22, President Trump and HHS Secretary Kennedy announce made the long-awaited announcement on autism that was the bold departure from previous failures to look squarely at the issue and speak boldly and honestly about it. And these two publicly funded officials boldly managed to ignore the entire herd of elephants in the room with them. Every. Single. One.
We have three bold new initiatives that sidestep the real issue as a means to “restore trust” and help families. ‘wanna buy a bridge?
But reality is rolling out, whether Kennedy and Trump want it to or not. Science is pumping out important, often very large-scale studies showing that mRNA vaccines are perhaps the greatest threat to humanity that we have ever faced.
There is good science emerging, but there is little good news in the remarkable document that follows here. The news, although mostly not good, is information nonetheless that you urgently need. CMN News, the Credible Medical News Network, provides a compendium and compilation of peer reviewed studies and authoritative opinion pieces which is, taken together, extremely worthwhile.
But the bad news is that the mRNA news is very, very bad. Not hopeless, but bad. Turbo cancer bad. VAIDS bad. Post injection DNA modification bad. Neurodegenerative and cardiovascular and immune function bad.
If you know people who are beginning to take in data to counter their blind faith in “safe and effective” magic words, there is a good deal here for them. Read on.
In case you needed something else to cement your conviction that mRNA vaccines are not good for living things (are any vaccines good for living things?), please take a look at this very large South Korean study.
What it underscores, yet again, is that no sane person will willingly accept an mRNA vaccine in their body, or that of their child/pet/loved one.
But isn’t Secretary Kennedy, our man on the Hill, protecting us from mRNA and other vaccines?
Among the “vaccines” approved since Secretary Kennedy took office on February 13, 2025, are more mRNA jabs, including a replicon one. And that is, indeed, very, very bad.
Here’s the list of approvals since then (mRNA jabs are in BOLD)
Penmenvy (GSK) was Approved on February 14, 2025. Nuvaxovid (Novavax) was approved May 19, 2025 mNexSpike (Moderna) was approved on May 30, 2025.2 This is a self-amplifying mRNA (replicon) vaccine which uses a self-replicating RNA platform that amplifies antigen expression inside cells. mResvia (Moderna) was approved June 12, 2025 Imovax (Sanofi) was approved on July 24, 2025 Ixchiq (Valneva Austria GmbH) was approved on August 6, 2025 Updated 2025-21026 COVID-19 formulations (Comirnaty by Prizer, Spikevax by Moderna and nNexSpike by Moderna) were approved August 27, 2025
Frankly, when you look at the other vaccines in this list, their lack of safety and dangerous profiles are appalling as well, but mRNA vaccines, especially the horrifying replicon platform ones, are an especial threat to the continued existence of humanity. Which makes sense, after all, since they are, in fact, bioweapons.
They are absolutely safe and effective,just not the way you think: safe for the people who developed them and hide behind the clever cover story of the weapons as vaccines and effective in incapacitating and killing people (that is what weapons are supposed to do, after all).
Not safe as in harmless and effective in preventing disease. Nope. Safe from prosecution and effective as destroying the population.
But, c’mon! We don’t have nearly enough of these Safe and Effective biological Molotov cocktails. We need more, lots more! We are in luck! Coming right up!
Here is a chart showing the jabs currently in the pipeline for FDA approval or recently approved. Note that we now have both “Conventional” mRNA and “Replicon mRNA” “vaccines” coming at us:
Secretary Kennedy and President Trump chose to focus on Tylenol (acetaminophen) as the convenient autism boogey man of the moment. Aside from a few dropped hints by the NOT Secretary of Health and Human Services, vaccines pretty much got a free pass despite Secretary Kennedy’s prior research, campaigns, statements, documentaries, law suites and speeches. Poof! Just like that!
It’s Tylenol! Secretary Kennedy’s research, campaigns, statements, documentaries, law suites and speeches, like the morning mist, seem to have vanished into our fondest memories of yesteryear.
Here is a question for Secretary Kennedy: now that we’ve got autism out of the way by just avoiding a simple OTC drug in pregnancy (which hardly explains the normally developing child who gets an MMR shot at 18 months and develops regressive autism over the next 24 hours, especially if they did not get Tylenol, but, never mind – we’re sticking to the Tylenol story), could we turn to the excess deaths, myocarditis, turbo cancers, the fertility cataclysm, clotting disorders (in life and in death), autoimmune diseases, neurodegenerative disorders and the host of other horrifying consequences of “Conventional” mRNA, the disastrous “Replicon” mRNA and the ordinary disaster that “ordinary” vaccines are and have been? Or do we get to focus on another major candidate making America unhealthy, like FDA Red Dye #3 or Tylenol?
Shot hijacks human cells to churn out “heterotrimeric” hybrid spikes—Frankenstein chimeras made of Wuhan and Omicron parts never found in nature.
A new preprint published August 19, 2025, in bioRxiv reveals that a Gates Foundation–funded team at Caltech, Gladstone Institutes, and Acuitas Therapeutics has engineered a self-amplifying mRNA vaccine platform that doesn’t just code for spike protein—it forces human cells to self-replicate the RNA instructions and churn out entire enveloped coronavirus-like particles (eVLPs).
Who & Where
The study was conducted by Chengcheng Fan, Alexander A. Cohen, Kim-Marie A. Dam, Annie V. Rorick, Ange-Célia I. Priso Fils, Zhi Yang, Priyanthi N. P. Gnanapragasam, Luisa N. Segovia, Kathryn E. Huey-Tubman, Woohyun J. Moon, Paulo J.C. Lin, Pamela J. Bjorkman, and Magnus A. G. Hoffmann, with affiliations at Caltech, Gladstone Institutes (UCSF), University of Washington, UC Berkeley, and Acuitas Therapeutics in Vancouver.
Funding disclosures make it explicit:
“These studies were funded by … Gates Foundation INV-034638 (P.J.B.) and INV-056219 (M.A.G.H.).”
That means Bill Gates’ foundation bankrolled this self-amplifying virus-factory vaccine.
Self-Amplifying & Whole Virus Design
Unlike first-generation COVID shots, this platform is designed to keep copying itself inside the cell—leading to higher, longer-lasting output.
Self-amplifying vaccines not only instruct the body’s cells to make the coronavirus spike protein—like the original mRNA COVID vaccines do—but they also instruct cells to make an enzyme that makes “copies of the original strand of RNA.”
This process leads to the production of even more spike protein within the body than first-generation mRNA COVID jabs produce.
Purported “benefits” of samRNA include extended duration (time) and magnitude (amount) of spike protein creation, a “strong” immune response, and requiring a smaller dose than original mRNA jabs.
The new study comes on top of Yale University School of Medicine’s discovery that spike protein from the original jabs can linger in the body for 709 days—when, earlier in the COVID pandemic, health authorities told us the spike protein only stays in the body “up to a few weeks.”
The authors of the new Gates-funded preprint describe their work this way:
“We recently developed the ESCRT- and ALIX-binding region (EABR) mRNA vaccine platform, which encodes engineered immunogens that induce budding of enveloped virus-like particles (eVLPs) from the plasma membrane, thereby resulting in presentation of immunogens on cell surfaces and eVLPs.”
This means the injected RNA doesn’t just make spike once—it replicates, keeps instructing, and drives cells to bud off whole coronavirus-like shells.
Far more viral material is created inside the body compared to regular mRNA jabs.
The implication: If standard mRNA already triggered spike toxicity and DNA contamination concerns, self-copying versions exponentially magnify those risks.
Cells Turned Into Virus Factories
The experiments confirmed that mammalian cells, when hit with this design, shed whole synthetic viral particles:
“To verify that the designed constructs induce eVLP budding, HEK293T were transiently transfected … After 48 hours, transfected cell supernatants were harvested, and eVLPs were purified by ultracentrifugation.”
Translation: In the lab, the vaccine instructions reprogrammed cells to manufacture and release entire pseudo-coronaviruses.
Novel Hybrid Spikes Created
Even more alarming, when two versions of spike were included (Wuhan + Omicron), they fused into brand-new hybrid proteins:
“Co-expression of ancestral Wu1 and Omicron S in the same cell could result in the formation of S heterotrimers consisting of Wu1 and Omicron S protomers.”
That means the vaccine doesn’t just make past spikes—it fabricates chimeric coronavirus spikes never seen before in nature.
Confirmed by Cryo-EM
This wasn’t theoretical modeling.
Cryo-electron microscopy reportedly directly showed the new synthetic hybrids:
“Single-particle cryo-EM analysis confirmed … trimerized HT2 and HT3 S proteins … These data demonstrate heterotrimeric S formation for soluble forms of SARS-CoV-2 S proteins.”
In other words, scientists actually imaged the new hybrid coronavirus spikes generated by the vaccine platform.
The Bigger Picture
This Gates-funded research is not isolated.
As my previous investigations have shown, governments and global foundations are already bankrolling self-amplifying mRNA (sa-mRNA) platforms worldwide.
Japan has already approved one (ARCT-154), and the Biden administration handed Gritstone Bio a $433-million contract to advance its own self-copying jab.
These vaccines are said to be “more efficient.”
But the reality is they extend duration and magnitude of spike production inside the body.
Cambridge University scientists already warned that first-gen mRNA is misread 10% of the time, producing rogue proteins in one-third of recipients.
If self-amplifying vaccines magnify those errors, the risks grow exponentially.
Bottom Line
Gates Foundation money funded an mRNA vaccine that self-replicates and programs cells to manufacture entire coronavirus-like particles.
This goes far beyond spike: cells become virus factories, producing synthetic hybrid spikes never found in nature.
Combined with the self-amplifying mechanism, the body isn’t just briefly making spike—it’s pushed into prolonged production of whole pseudo-viruses.
Bill Gates’ fingerprints are now on a technology that forces the body to churn out entire synthetic coronaviruses, amplified from within.
A new peer-reviewed study published today in Autoimmunityhas confirmed that both Pfizer-BioNTech and Moderna’s mRNA COVID-19 injections are contaminated with enormous quantities of DNA fragments—billions to hundreds of billions per dose—with Pfizer’s product uniquely containing the SV40 promoter-enhancer, a viral genetic element long associated with cancer concerns.
The study was authored by Dr. David J. Speicher, Dr. Jessica Rose, and Dr. Kevin McKernan.
The startling findings come as Pfizer’s own confidential safety data show serious injuries clustering in blood, immune, and neurological systems—the exact three human DNA fragments built into its vaccine plasmid, raising the possibility that plasmid integration is driving the very harms now dominating the safety signal.Subscribe
If you value this reporting, consider upgrading to a paid subscription.
Residual DNA Found in Every Vial Tested
The contamination was not limited to a few batches.
The authors make it plain:
“Residual DNA was detected in all 32 vaccine vials surveyed.”
Every single dose they tested had measurable DNA contamination.
Levels Exceed FDA & WHO Limits by Up to 627-Fold
The FDA and WHO set a maximum limit of 10 ng of DNA per dose.
These vaccines blew through that ceiling:
“Using fluorometry coupled with RNase A digestion, all products tested exceeded the guidelines for residual DNA set by the FDA and WHO of 10 ng/dose by 36–627-fold.”
Translation: These vaccines didn’t just skirt the limit—they shattered it, with up to 627 times more DNA than allowed.
Pfizer Contains SV40 Promoter—Linked to Gene Activation & Cancer
One of the most alarming discoveries: only Pfizer vials contained the SV40 promoter-enhancer, a sequence designed to push DNA into cell nuclei and drive gene expression.
“The SV40 promoter-enhancer-ori (0.25–23.72 ng/dose) was only detected in Pfizer vials.”
The SV40 promoter is not an inert bystander—it’s a nuclear targeting element used in gene therapy and flagged in past studies as tumorigenic.
This means Pfizer doses deliver cancer-linked viral DNA elements directly into patients’ cells, wrapped in lipid nanoparticles.
Billions to Hundreds of Billions of DNA Fragments Per Dose
This isn’t just a little DNA dust.
We’re talking staggering numbers:
“These data demonstrate the presence of 1.23 × 10^8 to 1.60 × 10^11 plasmid DNA fragments per dose encapsulated in lipid nanoparticles.”
That’s hundreds of billions of DNA molecules in each injection, not floating free but packaged in lipid nanoparticles designed to deliver genetic material into human cells.
Pfizer’s DNA Exceeds Limits in Multiple Lots
While Moderna’s DNA fragments stayed within FDA limits by qPCR, Pfizer repeatedly broke through:
“When tested by qPCR, all Moderna vials were within the regulatory limit, but 2/6 Pfizer lots (3 vials) exceeded the regulatory limit for the SV40 promoter-enhancer-ori by 2-fold.”
So Pfizer’s contamination isn’t hypothetical—it’s verified above-regulatory limits.
DNA Fragments Are Protected, Not Degradable
If these were just naked DNA fragments, they’d be destroyed quickly.
But because they’re wrapped inside lipid nanoparticles, they’re shielded from breakdown and can enter cells efficiently.
The authors stress:
“This study emphasizes the importance of methodological considerations when quantifying residual plasmid DNA in modRNA products, considering increased LNP transfection efficiency, and cumulative dosing presents significant and unquantified risks to human health.”
Layman’s terms: these DNA fragments are protected, designed to get into your cells, and regulators never accounted for that risk.
Authors’ Warning
In their conclusion, the authors reaffirm the data “demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in the modRNA COVID-19 products tested.”
They warn that current safety guidelines are outdated and must be revised, urging replication of their findings under strict forensic conditions.
“Our findings extend existing concerns about vaccine safety and call into question the relevance of guidelines conceived before the introduction of efficient transfection using LNPs. With several obvious limitations, we urge that our work is replicated under forensic conditions and that guidelines be revised to account for highly efficient DNA transfection and cumulative dosing.”
The scientists stress that regulators must follow the precautionary principle, prove safety with transparency, and fully disclose how these products are made.
“This work highlights the need for regulators and industry to adhere to the precautionary principle and provide sufficient and transparent evidence that products are safe and effective, and disclose the details of their composition and method of manufacture.”
Bottom Line
Pfizer and Moderna’s COVID-19 vaccines were found to contain massive amounts of residual DNA—far above regulatory thresholds—with Pfizer uniquely contaminated by SV40 promoter-enhancer sequences.
These DNA molecules are packaged in lipid nanoparticles that maximize cell entry, raising the specter of genome integration, cancer risk, and long-term genetic damage.
The authors—Speicher, Rose, and McKernan—are clear: regulators need to reassess DNA safety limits in light of lipid nanoparticle delivery and cumulative dosing, something never done before these products were unleashed globally.
I am expert in influenza, and have consulted with the WHO over the past two decades on the topic of flu vaccines. This is one subject matter I am extremely knowledgeable about. This goes back to my medical school days, when I worked with Robert Lamb, one of the top influenza virus specialists in the world. It extended through much of my career, including my serving as Director of Clinical Influenza Vaccine Research for Solvay Biologicals, in which I oversaw over $200 million in federal (BARDA) alternative (cell-based) influenza vaccine research funding.
What is happening now with “Bird flu” is another psyops campaign being conducted by the administrative/deep state, apparently in partnership with Pharma, against the American people. They know and we know that the “vaccines” being produced will be somewhat ineffective, as all flu “vaccines” are. The government is chasing a rapidly evolving RNA virus with a syringe, just like they did with HIV and Covid-19.
Generally, the currently circulating avian influenza strain in the US does not include any cases of human-to-human transmission. And the current mortality, with over 60 cases identified, is 0%. NOT 50%.
All the while they are getting prepared to roll out masks, lockdowns, quarantines, etc.
All the while getting ready to roll out mRNA vaccines for poultry and livestock, as well as for all of us.
The more they test, the more “Bird flu” (H5N1) they will find. This “pandemic” is nothing more than an artifact of their newly developed protocols to test cattle, poultry, pets, people, and wildlife on a massive scale for avian influenza. In years past, this was not even considered. In the past, the USG did fund a massive testing and surveillance program called “Biowatch.” That program was a colossal failure and a massive waste of money. Billions of dollars.
Of course, these facilities producing the tests have been repurposed from the Covid-19 testing facilities.
Key questions include:
Will we all comply?
Will we be forced to comply?
Will President Trump go along with the PsyWar/psyops campaign again?
We will know soon enough.
As the United States is testing everyone who has even the mildest symptoms for the H5N1 (avian) influenza, guess what – they are finding it! This is what we call in the lab, a “sampling bias.”
Globally, from 1997 until the present, there have been 907 reported cases of H5N1. And in fact, this particular outbreak was not the worst – and it is the only one where a massive testing campaign has occurred. It appears that this is partly due to the new diagnostic capabilities developed and deployed during Covid-19. The more you test, the more you find. But is it clinically significant?
The Case Study of Tetanus: Supply Chain Issues.
The CDC recommends a booster for the tetanus vaccine every 10 years for adults.
However, research published almost a decade ago suggests that the protection from tetanus and diphtheria vaccination lasts at least 30 years after completing the standard childhood vaccination series.
“We have always been told to get a tetanus shot every 10 years, but actually, there is very little data to prove or disprove that timeline. When we looked at the levels of immunity among 546 adults, we realized that antibody titers against tetanus and diphtheria lasted much longer then previously believed.”
-Mark K. Slifka, Ph.D, study author
This research, published in a highly reputable journal, suggests that a revised vaccination schedule with boosters occurring at ages 30 and 60 would be sufficient. As this was published in early 2016, the US government, at the very least, could have commissioned easily designed prospective and retrospective studies to confirm these results. And those results would have been published by now, with the tetanus adult schedule revised to reflect what is now known about the durable immunity of tetanus and diphtheria vaccines. Reducing the boosters to just two shots would save the government vast sums of money.
Not only that, but both the tetanus and diphtheria vaccines carry risks for adults. It is estimated that 50%–85% of patients experience injection site pain or tenderness, 25%–30% experience edema and erythema. Higher preexisting anti-tetanus antibody levels are also associated with a higher reactogenicity rate and greater severity (reference).
Anaphylaxis after tetanus vaccination represents a rare but potentially serious adverse event, with an incidence of 1.6 cases per million doses. That means if 100 million adults receive the booster every ten years, 320 cases of anaphylaxis will be avoided over the 30-year period – from those two boosters being eliminated. Tetanus has always been a “rare” disease, spread through a skin wound contaminated by Clostridium tetani bacteria, commonly found in soil, dust, and manure. Before vaccines were available, there were about 500 cases a year, with most resulting in death. Concerns about vaccine-associated adverse events when immunizations were performed at short intervals led to a revision of the tetanus/diphtheria vaccination schedule in 1966 to once every 10 years for patients >6 years of age.
It has recently come to my attention that the traditional stand-alone tetanus vaccine (TT) that one used to receive as an adult has been discontinued due to WHO recommendations. Their reasoning being:
Use of TTCV combinations with diphtheria toxoid are strongly encouraged and single-antigen vaccines should be discontinued whenever feasible to help maintain both high diphtheria and high tetanus immunity throughout the life course.
The CDC blames the shuttering of the only plant producing TT for the current lack of a stand-alone TT vaccine.
Now, in order to get a booster tetanus shot, an adult must take the following.
Td: Sanofi’s Tenivacprotects against tetanus and diphtheria. Given to people 7 years and older as a booster every 10 years. *A version also includes pertussis (eg DPT), but due to the risk of encephalitis, it is not recommended as a booster.
Why is the DPT combination vaccine discouraged in adults due to encephalitis risk, but is it recommended for children? Another one of those inconvenient issues that plague the CDC-recommended childhood vaccine schedule.
While supplies of diphtheria, tetanus, and pertussis (Tdap) vaccines (Sanofi’s Adacel and GSK’s Boostrix) aren’t limited, they are more expensive, and a very small fraction of patients can develop encephalopathy (brain damage) from the pertussis component.
In the United States, diphtheria is virtually non-existent, with only 14 cases reported between 1996 and 2018. Of those cases reported, most were from international travelers or immigrants.
The market for a stand-alone TT vaccine vanished worldwide due to WHO recommendations to stop the sales of the TT vaccine. Which was due to the relatively few, economically stressed countries where diphtheria is still an issue. So, therefore, the only facility manufacturing the TT vaccine was shut down within the last year.
The blowback from the WHO recommendations is that now there is a shortage of tetanus and diphtheria (Td) vaccine in the United States, according to the Centers for Disease Control and Prevention (CDC) website.
This all comes down to poor planning. And illustrates why supply chain issues and infectious disease countermeasure stockpiles are essential considerations for governments.
The good news is that unless one is immunosuppressed, most of us have almost lifelong immunity against tetanus and diphtheria.
My recommendation is that unless one gets a very deep and dirty puncture wound and has not had a tetanus shot in over ten years or longer, avoid that booster.
Here is the ugly secret about influenza vaccines. They are given to protect one group of vulnerable people. Those who are immunosuppressed, and that cohort includes the very elderly.
If those influenza vaccine manufacturing plants only make enough vaccines for those susceptible to a severe case of the flu, there would not be enough of a market to sustain their production costs. Furthermore, if there were a pandemic of some sort of highly pathogenic influenza, there would not be sufficient capacity to make enough vaccines to meet demand.
Egg-based influenza vaccine production requires super “clean” eggs; about 100 million “clean” fertilized eggs are needed annually for vaccine production in the US alone. Candidate vaccine viruses are injected into the eggs. If the process is shuttered, the whole production comes to a screeching halt. Many vaccines can be stored for long periods. Even as long as a decade. This stockpiling system works well for DNA viruses with a low mutation rate. Stockpiling is rarely a solution for vaccines developed for RNA viruses that mutate rapidly.
Therefore, the influenza vaccine is pushed on the American people year after year. As a way to maintain “warm base manufacturing” and ensure sufficient market size to support industrial operations.
I have spoken on this subject at the WHO and US government agencies, as well as many, many conferences. Unfortunately, because the mRNA and RNA vaccine platforms require a lot of freezer space (commonly -20°C) to stockpile for even short periods, this limits the ability to stockpile. Furthermore, the frozen storage requirements are only for up to 6 months. That means stockpiling for more extended storage is not currently done, and it is back to square one on the supply chain issue.
The issue with freezer space and mRNA vaccines is one that most likely won’t be solved. This benefits the manufacturers of this vaccine technology – the US government has an endless need for new vaccines as the old ones expire.
My small hope is that the mRNA platform will be too costly to justify its continued use, as appeals concerning safety (or lack of) seem to fall on deaf FDA ears.
In the meantime, don’t believe the hype generated by ex-officials from the Biden and Trump administrations.
Both Dr. Lena Wen, CNN correspondent, and Dr. Redfield, ex-director of the CDC, have gone on to mainstream media shows and promoted the narrative that the case fatality rate for avian influenza is over 50 percent. This, frankly, is a lie that the WHO is promoting. Bird flu generally is not tested for when someone has flu symptoms. When an outbreak of avian flu occurs on a poultry farm, testing of farm workers who are seriously ill will commence. This has led to the generation of the 890 case reports since 2003. Of those seriously ill patients reported to the WHO, over 50 percent died.
This is not an actual case fatality rate of avian flu around the world. It is, again, a sampling error due to a tiny data set derived from those who are at greatest risk due to general health. And just like the WHO reported on an exaggerated case fatality rate for mPOX, which was also based on a sampling error, or for Covid-19, again a sampling error, it is now used to justify psychological bioterrorism on the world population. Please don’t fall for it.
El Gato Malo on X succinctly points out that Dr. Leana Wen and her public health ilk are advancing:
1. Do more of the same lousy testing used in Covid-19 to overstate a disease and cause panic.
2. Develop another non-sterilizing non-vaccine that does not work to be pushed on “the vulnerable.”
3. Doing it “right now” under EUA, so whoever makes these tests and jabs can cash in and be shielded from liability.
4. Claiming that proxies like “triggers antibody production” demonstrate clinical clinical efficacy.
It’s just one last smash-and-grab for cash before the Brandon administration ends. Anyone who falls for this one will truly fall for anything.
Question: what are Leana’s conflicts of interest? Who is paying her or giving her grants?
For those that haven’t viewed Dr. Redfield speaking of the avian flu case fatality rate, have a watch below. It is genuinely shocking. This fear-mongering comes from an ex-director of the CDC. Shame on him.
Frankly, it reminds me of the 51 intelligence officials claiming that Hunter Biden’s laptop was fake.
One has to wonder what conflict of interest motivated him to say this on national TV?
Remember in the US, there have been 62 cases of avian influenza discovered, and all but one case were very mild.
This deep dive into the supply chain issues is meant to show that public health has put itself into a groupthink situation that it can’t escape.
Many solutions to this quandary do not involve an evermore expanding schedule of vaccinations, stockpiled for some future use. I have some general thoughts before I sign off.
The use of early treatments via safe, proven drugs is a good solution.
We now have many antibiotics to treat bacterial infections. Vaccines do not always need to be our first defense.
Our medical system is very good at treating infectious diseases. The risks from such diseases are much less than it once was. People do not have to live in fear of infectious disease. I like to ask people, how many people do you know have died of flu? If you know of any (I don’t), how old were they?
The need to scare people into more and more vaccines is a dangerous trend.
And yes, the more vaccinations one receives, the more likely an adverse event.
Vaccinating pregnant women and babies should always be a last resort.
It is time for Congress to rethink the vaccine liability laws.
No matter how bad you think Covid policies were, they were intended to be worse.
Consider the vaccine passports alone. Six cities were locked down to include only the vaccinated in public indoor places. They were New York City, Boston, Chicago, New Orleans, Washington, D.C., and Seattle. The plan was to enforce this with a vaccine passport. It broke. Once the news leaked that the shot didn’t stop infection or transmission, the planners lost public support and the scheme collapsed.
It was undoubtedly planned to be permanent and nationwide if not worldwide. Instead, the scheme had to be dialed back.
Features of the CDC’s edicts did incredible damage. It imposed the rent moratorium. It decreed the ridiculous “six feet of distance” and mask mandates. It forced Plexiglas as the interface for commercial transactions. It implied that mail-in balloting must be the norm, which probably flipped the election. It delayed the reopening as long as possible. It was sadistic.
Even with all that, worse was planned. On July 26, 2020, with the George Floyd riots having finally settled down, the CDC issued a plan for establishing nationwide quarantine camps. People were to be isolated, given only food and some cleaning supplies. They would be banned from participating in any religious services. The plan included contingencies for preventing suicide. There were no provisions made for any legal appeals or even the right to legal counsel.
The plan’s authors were unnamed but included 26 footnotes. It was completely official. The document was only removed on about March 26, 2023. During the entire intervening time, the plan survived on the CDC’s public site with little to no public notice or controversy.
It was called “Interim Operational Considerations for Implementing the Shielding Approach to Prevent COVID-19 Infections in Humanitarian Settings.”
“This document presents considerations from the perspective of the U.S. Centers for Disease Control & Prevention (CDC) for implementing the shielding approach in humanitarian settings as outlined in guidance documents focused on camps, displaced populations and low-resource settings. This approach has never been documented and has raised questions and concerns among humanitarian partners who support response activities in these settings. The purpose of this document is to highlight potential implementation challenges of the shielding approach from CDC’s perspective and guide thinking around implementation in the absence of empirical data. Considerations are based on current evidence known about the transmission and severity of coronavirus disease 2019 (COVID-19) and may need to be revised as more information becomes available.”
By absence of empirical data, the meaning is: nothing like this has ever been tried. The point of the document was to map out how it could be possible and alert authorities to possible pitfalls to be avoided.
The meaning of “shielding” is “to reduce the number of severe Covid-19 cases by limiting contact between individuals at higher risk of developing severe disease (‘high-risk’) and the general population (‘low-risk’). High-risk individuals would be temporarily relocated to safe or ‘green zones’ established at the household, neighborhood, camp/sector, or community level depending on the context and setting. They would have minimal contact with family members and other low-risk residents.”
In other words, this is what used to be concentration camps.
Who are these people who would be rounded up? They are “older adults and people of any age who have serious underlying medical conditions.” Who determines this? Public health authorities. The purpose? The CDC explains: “physically separating high-risk individuals from the general population” allows authorities “to prioritize the use of the limited available resources.”
This sounds a lot like condemning people to death in the name of protecting them.
The model establishes three levels. First is the household level. Here high-risk people are“physically isolated from other household members.” That alone is objectionable. Elders need people to take care of them. They need love and to be surrounded by family. The CDC should never imagine that it would intervene in households to force old people into separate places.
The model jumps from households to the “neighborhood level.” Here we have the same approach: forced separation of those deemed vulnerable.
From there, the model jumps again to the “camp/sector level.” Here it is different. “A group of shelters such as schools, community buildings within a camp/sector (max 50 high-risk individuals per single green zone) where high-risk individuals are physically isolated together. One entry point is used for exchange of food, supplies, etc. A meeting area is used for residents and visitors to interact while practicing physical distancing (2 meters). No movement into or outside the green zone.”
Yes, you read that correctly. The CDC is here proposing concentration camps for the sick or anyone they deem to be in danger of medically significant consequences of infection.
Further: “to minimize external contact, each green zone should include able-bodied high-risk individuals capable of caring for residents who have disabilities or are less mobile. Otherwise, designate low-risk individuals for these tasks, preferably who have recovered from confirmed COVID-19 and are assumed to be immune.”
The plan says in passing, contradicting thousands of years of experience, “Currently, we do not know if prior infection confers immunity.” Therefore the only solution is to minimize all exposure throughout the whole population. Getting sick is criminalized.
These camps require a “dedicated staff” to “monitor each green zone. Monitoring includes both adherence to protocols and potential adverse effects or outcomes due to isolation and stigma. It may be necessary to assign someone within the green zone, if feasible, to minimize movement in/out of green zones.”
The people housed in these camps need to have good explanations of why they are denied even basic religious freedom. The report explains:
“Proactive planning ahead of time, including strong community engagement and risk communication is needed to better understand the issues and concerns of restricting individuals from participating in communal practices because they are being shielded. Failure to do so could lead to both interpersonal and communal violence.”
Further, there must be some mechanisms to prohibit suicide:
Additional stress and worry are common during any epidemic and may be more pronounced with COVID-19 due to the novelty of the disease and increased fear of infection, increased childcare responsibilities due to school closures, and loss of livelihoods. Thus, in addition to the risk of stigmatization and feeling of isolation, this shielding approach may have an important psychological impact and may lead to significant emotional distress, exacerbate existing mental illness or contribute to anxiety, depression, helplessness, grief, substance abuse, or thoughts of suicide among those who are separated or have been left behind. Shielded individuals with concurrent severe mental health conditions should not be left alone. There must be a caregiver allocated to them to prevent further protection risks such as neglect and abuse.
The biggest risk, the document explains, is as follows: “While the shielding approach is not meant to be coercive, it may appear forced or be misunderstood in humanitarian settings.”
(It should go without saying but this “shielding” approach suggested here has nothing to do with focused protection of the Great Barrington Declaration. Focused protection specifically says: “schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.”)
In four years of research, and encountering truly shocking documents and evidence of what happened in the Covid years, this one certainly ranks up at the top of the list of totalitarian schemes for pathogenic control prior to vaccination. It is quite simply mind-blowing that such a scheme could ever be contemplated.
Who wrote it? What kind of deep institutional pathology exists that enabled this to be contemplated? The CDC has 10,600 full-time employees and contractors and a budget of $11.5 billion. In light of this report and everything else that has gone on there for four years, both numbers should be zero.
















Recent Comments