Using “the same platform methods used for Pfizer’s COVID-19 and seasonal influenza mRNA vaccines.”
Researchers from the U.S. Centers for Disease Control and Prevention (CDC) and Pfizer Inc. have created new, engineered H5 bird flu influenza genetic constructs, including a codon-optimized hemagglutinin (HA) gene with a synthetically altered cleavage site, as documented in a Saturday npj Vaccines publication.
According to the authors, the stated purpose of the study was to evaluate an mRNA-based H5 vaccine, which they describe as “a nucleoside-modified mRNA construct encoding the full-length, codon-optimized HA protein with the polybasic cleavage site deleted from A/Astrakhan/3212/2020 A(H5N8).”
The paper confirms that the engineered HA used in the study was genetically modified beyond its purported natural form.
Cleavage Site Optimized
The authors state that the cleavage site was synthetically altered, writing that the polybasic amino acids were “mutated from ‘REKRRKR’ to ‘RETR’.”
The cleavage site is like a switch that must be cut to turn the flu pathogen “on” so it can infect cells, and if this site can be cut by many types of enzymes in the body, the virus can spread more and cause worse disease.
LNPs for mRNA Therapeutics
The engineered constructs were then formulated into lipid nanoparticles following “the same platform methods used for Pfizer’s COVID-19 and seasonal influenza mRNA vaccines.”
The work was conducted by multiple CDC branches, including the Influenza Division, the Division of High-Consequence Pathogens and Pathology, and the Office of Advanced Molecular Detection.
Pfizer Scientists at BSL-3 Lab
It was carried out by Pfizer scientists at the company’s Pearl River, NY facility, with additional involvement from ORISE.
The authors specify that “all research involving HPAI A(H5N1) viruses was conducted within Biosafety Level 3 enhanced (BSL-3E) or ABSL-3 facilities at the CDC.”
100% Transmission Rate
To test the performance of the engineered constructs, the CDC–Pfizer team conducted live-virus challenge experiments using human-derived H5N1 isolates.
The ferrets were infected with virus formations “A/Chile/25945/2023” and “A/Michigan/90/2024… from a farm worker exposed to infected cattle.”
Using these human isolates, the researchers documented efficient mammal-to-mammal spread, reporting a “100% transmission rate” in unvaccinated ferrets.
Funding & Conflicts of Interest
The funding disclosures indicate direct federal and corporate sponsorship.
The authors state: “This work was funded by the US Centers for Disease Control and Prevention and by Pfizer Inc.”
The authors also disclose full corporate participation in the scientific process, writing: “Pfizer was involved in the design, analysis, and interpretation of the data in these research studies, the writing of this report, and the decision to publish.”
Additionally, the paper notes that Pfizer researchers associated with the project are “inventors on patent applications relating to influenza mRNA compositions.”
Bottom Line
The new study documents that CDC and Pfizer jointly engineered new H5 constructs through codon optimization and cleavage-site mutation, formulated them using Pfizer’s mRNA-LNP platform, and then tested them against recent human H5N1 isolates inside CDC BSL-3E laboratories.
The result is a federally backed, corporate-driven program in which U.S. authorities and Pfizer quietly engineered H5 influenza genetics and tested them with human-infecting H5N1—blurring the line between vaccine development and high-risk pathogen manipulation.
The dangerous experiments raise national security concerns.
Amid worries of a coming avian influenza pandemic.
A new study preprint published last week in the journal npj Vaccines describes a multinational research program that designed, engineered, and tested synthetic versions of the H5N1 bird flu virus’s hemagglutinin protein—one of the key components that allows the virus to infect cells.
The scientists altered these genetic sequences, delivered them into animals using advanced DNA and lipid-nanoparticle (LNP) technologies, and then conducted lethal challenge experiments with highly pathogenic H5N1 viruses inside a Canadian government biocontainment facility.
This means researchers created synthetic versions of a dangerous flu component, injected them into mice using vaccine-style technologies, and then exposed the animals to very deadly strains of H5N1 to test how well the constructs worked.
The study is authored by a large team from the United States, Canada, and Europe, including researchers from the Wistar Institute, the University of Pennsylvania, the Public Health Agency of Canada, and the University of Bologna.
Funding Sources
The research was funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID) through its Collaborative Influenza Vaccine Innovation Centers (CIVIC) program under contract 75N93019C00051.
This is a federal vaccine-development initiative said to be designed to prepare the U.S. for future influenza outbreaks using rapidly adaptable genetic platforms.
But the creation of new viruses raises national security concerns.
Additional support came from the W.W. Smith Charitable Trust Distinguished Professorship in Cancer Research and The Jill and Mark Fishman Foundation.
In other words, the work was paid for by the same federal agencies responsible for pandemic vaccine programs, along with private biomedical foundations.
Institutions Involved
The experiments were carried out by a coordinated network of laboratories:
The Wistar Institute (Philadelphia) designed and built the synthetic H5N1 DNA constructs, performed immune studies, and conducted structural modeling using AlphaFold 3.
The University of Pennsylvania assisted with lipid-nanoparticle formulation and microbiology methods.
The Public Health Agency of Canada’s National Microbiology Laboratory in Winnipeg performed the live H5N1 infections and lethal challenge experiments, including tests using a recombinant H5N1 virus constructed from synthetic gene segments.
The University of Bologna contributed additional biotechnology expertise.
The U.S. labs designed and built the engineered genetic materials, and the Canadian government lab carried out the dangerous live-virus testing.
The authors include: Ebony N. Gary, Nicholas J. Tursi, Casey E. Hojecki, Robert Vendramelli, Martina Tomirotti, Bryce Warner, Cory Livingston, Thang Truong, Yangcheng Gao, Sachchidanand Tiwari, Norbert Pardi, Darwyn Kobasa, and senior author David B. Weiner.
What Is Scientifically Alarming
Several aspects of this research stand out as high-risk from a biodefense perspective, even though the work is framed as vaccine development.
1. Synthetic Genetic Engineering of H5N1 Components
The team did not merely study existing viruses.
They engineered new synthetic versions of the H5N1 hemagglutinin gene, including codon optimization (which boosts expression in human cells) and deliberate modification of the protease cleavage site, a region strongly linked to H5N1’s virulence.
They edited the part of the virus that helps determine how dangerous it is.
2. Construction of a Recombinant H5N1 Virus From Synthesized Gene Segments
The researchers created a chimeric H5N1 virus by combining gene segments that were commercially synthesized and assembled from cloned DNA.
They then rescued this artificial virus using reverse-genetics techniques.
This means they built a new lab-made version of H5N1, piece-by-piece, using artificial DNA.
3. Use of LNP Delivery and Electroporation to Express Viral Genes Inside Animals
The study delivered the synthetic HA genes using LNPs (the same technology used in COVID-19 mRNA vaccines) and electroporation, a technique that uses electrical pulses to force genetic material into cells.
Both approaches greatly increase how efficiently engineered genetic material can spread through tissues.
These tools make it much easier for lab-designed genetic material to take hold inside the body.
4. Lethal Challenge Work Using High-Dose H5N1
Mice were exposed to 10 times the lethal dose (10 LD50) of highly pathogenic H5N1 strains—including both natural isolates and the lab-built recombinant virus.
They infected animals with very large amounts of a deadly virus to test whether the synthetic constructs gave protection.
5. Corporate Ties of the Senior Author
The senior scientist, David B. Weiner, discloses paid relationships with Pfizer, AstraZeneca, Sanofi, Inovio, Flagship, and others.
This means the research directly intersects with large pharmaceutical companies that develop genetic vaccines and related technologies, raising conflicts of interest worries.
Why This Matters for Policymakers
This study demonstrates that federal funding is supporting research with clear dual-use potential, meaning it could advance vaccines or, if misapplied, enable the construction or enhancement of dangerous influenza viruses.
The same techniques used to create synthetic vaccine antigens—codon optimization, cleavage-site modification, LNP delivery, and recombinant virus assembly—can also be used to create novel viral strains with properties that do not currently exist in nature.
The technical sophistication is notable, especially the deliberate editing of cleavage sites and the full reconstruction of an H5N1 virus from cloned fragments, which is uncommon outside of specialized influenza-engineering programs.
This work shows that laboratories funded by the U.S. government and partnered with foreign agencies are actively engineering pieces of dangerous bird flu viruses and testing them in high-security facilities.
The stated goal is to develop better vaccines, but the methods overlap with techniques traditionally associated with gain-of-function research, which can create new biological risks if not tightly controlled.
A Thursday npj Vaccines study confirms U.S. federal agencies, including the U.S. Department of Agriculture (USDA) and the National Institutes of Health (NIH), funded the laboratory creation of genetically engineered two influenza viruses (H9N2/H5N2) built from plasmids, artificial gene fusions, synthetic insertions, and modified genome segments.
The work was carried out by researchers at the University of Georgia, the Icahn School of Medicine at Mount Sinai, and the U.S. National Poultry Research Center, Agricultural Research Service, USDA.
The authors listed on the study are: “Flavio Cargnin Faccin, L. Claire Gay, Dikshya Regmi, Robert Hoelzl, Teresa D. Mejías, Darrell Kapczynski, Florian Krammer & Daniel R. Perez.”
The study’s funding confirms direct federal involvement.
“Funding for this work includes grants… National Institute of Food and Agriculture (NIFA), U.S. Department of Agriculture (USDA) Grant award numbers 2021-67015-33406 and 2024-67015-42736, National Institute of Allergy and Infectious Diseases, National Institutes of Health (NIH) Contract number 75N93021C00014.”
Construction of the Engineered Viruses
The researchers did not isolate a purported virus from nature.
They built new viruses entirely through reverse genetics, using plasmid DNA transfected into human and dog cell lines.
The paper states: “Recombinant viruses were rescued by reverse genetics using the 8-plasmid system and helper plasmids in a coculture of HEK293T and MDCK cells.”
The process is described explicitly.
According to the authors, “1 µg of each plasmid was mixed… and used to overlay the cell coculture.”
Viral stocks were then expanded artificially rather than occurring naturally, as the study reports: “Viral stocks were generated in 10-day-old specific pathogen-free (SPF) eggs.”
These details confirm that the viruses were constructed in the laboratory, rescued from DNA, and amplified in eggs.
‘Chimeric’ Pathogens
The viruses created under USDA and NIH funding are laboratory-assembled chimeras—genomes stitched together from engineered parts that do not exist in nature.
The study shows that two influenza proteins were fused into a single artificial gene, something no wild virus carries.
As the authors write: “Segment 2 was modified to encode a chimeric PB1-M2 open reading frame (ORF) separated by a glycine-glycine-glycine-glycine-serine (G4S) spacer.”
This forces the virus to make an unnatural hybrid protein.
To ensure the virus depends on this man-made fusion protein, its normal version of M2 was deliberately shut off.
The paper states: “Segment 7 was modified by introducing multiple early stop codons in the M2 ORF via site-directed mutagenesis to prevent its expression.”
This eliminates the native M2 and locks the virus into the engineered design.
The researchers also inserted a synthetic 58–amino acid sequence into the HA segment, including an artificial peptide not found in any influenza strain.
The methods describe this as: “Segment 4… was modified to insert a 58-amino-acid-long sequence… which included the unique 8-amino-acid peptide… ‘DRPAVIAN.’”
Another modification swaps out the cleavage site of an H5 virus and replaces it with one taken from a human 1934 H1N1 strain, altering how the virus activates inside host cells.
The authors state: “The H5 HA HPAI cleavage site was replaced with that of the A/Puerto Rico/8/1934 (H1N1) (PR8) strain.”
Finally, the virus was engineered to manufacture a chicken immune-signaling molecule from inside infected cells.
The study confirms: “The mature protein-coding sequence of chicken IL-18… was subcloned in frame with the NA ORF.”
These combined changes—fusion genes, disabled native proteins, synthetic inserts, human-strain cleavage sites, and cytokine-expression modules—create a virus with properties that no purported natural influenza lineage carries.
Aerosol Exposure in Animals
The researchers then exposed day-old chickens to the engineered viruses through aerosolized live-virus delivery.
The methods describe this process clearly, all done within BSL-3 lab conditions:
“One-day old SPF White Leghorn chickens… were vaccinated via aerosol using an aerosol chamber… A 5 mL volume of MLV-H9N2-IL was loaded into the Aeroneb lab nebulizer, resulting in an average exposure of 1×10⁶ EID50/chicken… The exposure lasted for 15 min.”
This confirms that the USDA- and NIH-funded engineered viruses were not only constructed but also introduced into animals through airborne delivery.
Bottom Line
The study documents how U.S. federal agencies oversaw the full laboratory assembly of engineered influenza viruses—built from plasmids, redesigned through reverse genetics, and altered with fusion genes, stop-codon knockouts, synthetic peptide insertions, cytokine-expression modules, and foreign cleavage sites.
These are not environmental isolates; they are fully man-made constructs created inside U.S. government and university laboratories under USDA and NIH funding.
The viruses were then delivered to live animals by aerosol, demonstrating not only construction capability but functional deployment.
Work of this nature carries obvious national-security implications: it establishes the technical capacity to design, modify, and disseminate engineered influenza strains whose properties cannot be predicted from any purported natural lineage.
In a stunning exchange on the PBD Podcast (Episode 690), U.S. Commissioner of Food and Drugs (FDA) Dr. Marty Makary, a Johns Hopkins surgeon, dropped two bombshell admissions about pathogen origins—one about HIV, the other about Lyme disease.
Dr. Makary openly entertained the possibility that HIV “may very well have come from a lab in Africa,” saying the film Thank You, Dr. Fauci “explore[s] a non-traditional narrative, which has not gotten the attention it deserves.”
HIV (Human Immunodeficiency Virus) is said to be a retrovirus that targets and destroys CD4 T cells in the immune system, weakening the body’s ability to fight infections and potentially leading to AIDS if untreated.
When asked where Lyme disease originated, Makary answered directly: “I can tell you with a high degree of probability. It came from Lab 257 on Plum Island.”
Lyme disease is a bacterial infection caused by Borrelia burgdorferi, transmitted through bites from infected blacklegged ticks, often marked by an expanding “bull’s-eye” rash, fever, fatigue, and joint pain.
The head of the FDA has admitted that two major diseases originated not in nature, but in government laboratories, raising questions about other disease origins.
HIV: ‘It May Very Well Have Come from a Lab in Africa’
Makary described how mainstream institutions avoid uncomfortable evidence about HIV’s beginnings.
When pressed on the origin of AIDS, he said the following:
“They explore a non-traditional narrative, which has not gotten the attention it deserves. And that is that it may very well have come from a lab in Africa.”
Makary is one of the most publicly visible medical figures in the United States—Hopkins professor, long-time NIH-funded surgeon, and prominent FDA advisor.
His admission directly contradicts decades of official insistence that HIV was unquestionably a zoonotic spillover.
Lyme Disease: ‘It came from Lab 257 on Plum Island’
When the conversation turned to Lyme disease—which afflicts millions of Americans—Makary said:
“I can tell you with a high degree of probability. It came from Lab 257 on Plum Island just outside of Connecticut, 25 miles from Lyme, Connecticut, where the first case was described.”
He then explained how he knows:
“First of all, you can read the book Bitten. It’s a great book.”
And he explained who the U.S. brought to Plum Island after WWII:
“When the Nazi war criminal doctors were executed in Nuremberg, at least one of them was spared and brought to the United States so that his mind could be used by the US military for so-called Biodefense. And they put him on Plum Island and he had said very openly that he believed an incredible form of biowarfare was infecting ticks. And that that’s what Lyme disease is.”
Makary is referring to the notorious Erich Traub, the Nazi bioweapons scientist recruited by U.S. military intelligence.
“A bunch of mad scientists doing things… How many physicians know that it came from Lab 257? Approximately 1%.”
He ended with the warning that the public health establishment refuses to confront:
“Just because you can do something doesn’t mean you should do it. And sometimes we can cause more harm than we can good by messing with Mother Nature.”
Once the FDA commissioner concedes that two major diseases came from government labs, the narrative of “natural outbreaks” collapses on its own.
The only thing left to find out is how far these patterns go.
As countries engineer avian influenza bird flu pathogens without restraint.
The World Health Organization and Egypt’s Ministry of Health just completed a national-scale workshop training nearly 300 surveillance officers to expand real-time monitoring of influenza and other respiratory pathogens across the country.
The move comes as this website has been tracking multiple governments performing gain-of-function experiments on avian influenza “bird flu” pathogens (see below this article), raising worries of another orchestrated, man-made pandemic.
The WHO announcement frames the workshop as routine and annual, masking the scale of the expansion and the integration of surveillance functions under WHO guidance.
“The annual meeting and accompanying workshop on integrated surveillance of acute respiratory infections (ARIs), conducted by the Egyptian Ministry of Health and Population in collaboration with the World Health Organization (WHO) Country Office in Egypt, brought together around 270 public health professionals.”
More than a simple “meeting,” this represents a consolidation of a national respiratory surveillance grid.
Two hundred and seventy surveillance officers trained at once sounds more like a deployment than a workshop.
The framing as “annual” makes the expansion appear normal and non-threatening when, in reality, it marks a significant expansion of WHO’s operational footprint inside Egypt’s health system.
Thirty Sentinel Sites Feeding a Unified National Surveillance Grid
The announcement identifies the personnel being trained, revealing a full-spectrum surveillance workforce (epidemiology, clinical staff, data specialists) rather than a narrow set of influenza experts.
“The participants, all involved in surveillance, included epidemiologists, data officers, physicians, nurses and laboratory specialists drawn from 30 ARI sentinel sites across 15 governorates.”
This proves the surveillance integration is nationwide.
“Sentinel sites across 15 governorates” means Egypt’s surveillance network is now being unified under a single reporting system.
Bringing in data officers signals the transition to real-time digital surveillance and automated reporting pipelines that feed directly into WHO’s global systems.
A Surveillance Framework That Never Powers Down
The WHO announcement reveals the core mission: strengthen surveillance for influenza and all respiratory viruses—not limited to outbreaks or emergencies.
“The sessions aimed to strengthen national capacities in disease surveillance for influenza and other respiratory viruses and improve preparedness for respiratory disease threats, particularly those with pandemic potential.”
They want to treat all respiratory viruses—seasonal or otherwise—as potential triggers for global coordination.
The phrase “other respiratory viruses” quietly expands surveillance beyond influenza to include COVID, avian flu, MERS, and any future pathogen, making continuous monitoring the norm.
This is how perpetual surveillance infrastructures are justified.
The workshop covers multiple pathogen classes, including zoonotic viruses, merging animal-origin threats with routine respiratory surveillance.
“The discussions covered a wide range of topics, including updates on the global and national epidemiological situation of influenza, COVID-19, avian influenza, Middle East respiratory syndrome coronavirus (MERS-CoV) and zoonotic respiratory infections.”
So the system is designed to take in constant “signal noise” from zoonotic sources—livestock, poultry, wildlife.
Zoonotic data is always active, which means alert conditions can always be justified.
Folding zoonotic viruses into human surveillance pipelines is a central feature because it guarantees a steady stream of “pandemic potential” warnings.
WHO Uses ‘Performance Evaluations’ to Enforce Surveillance Compliance
The announcement describes the unification and standardization of national operating procedures, indicating that Egypt’s surveillance mechanics are being aligned directly with WHO standards.
“Participants reviewed standard operating procedures for ARI and influenza-like illness (ILI) sentinel surveillance and laboratory operations, alongside findings from performance evaluations.”
The mention of “performance evaluations” means WHO is grading Egypt’s compliance with global surveillance standards.
The evaluations will serve as a mechanism for harmonizing Egypt’s protocols with WHO’s prescribed methods.
This is an oversight structure.
Once surveillance is standardized, WHO essentially co-authors the national surveillance workflow.
Building the Digital Backbone of a Permanent Respiratory Surveillance State
The WHO press release goes on to introduce the digital component—data integration, dashboards, and real-time reporting—showing that Egypt’s network is being plugged into a centralized digital surveillance architecture.
“They explored how digital tools and platforms can enhance ARI data quality and timeliness and discussed data reporting through the National Electronic Disease Surveillance System (NEDSS) and the ARI/ILI Power BI dashboard which are used to collect, analyse and visualize respiratory surveillance disease data.”
The system they’re describing allows centralized ingestion of respiratory data across Egypt, instant analytics, automatic WHO reporting, and algorithmic signal detection.
The Power BI dashboard represents the command interface of a national respiratory surveillance grid.
This is the infrastructure required for automated “health security” triggers, border protocols, and potential digital health certifications.
PRET: WHO’s Framework for Perpetual Surveillance, Now Active in Egypt
The WHO directly names PRET, acknowledging that Egypt is now being operationally aligned with WHO’s new global framework that replaces traditional outbreak response with permanent readiness.
“The sessions also covered WHO’s Preparedness and Resilience for Emerging Threats (PRET) framework, an innovative approach designed to improve countries’ pandemic preparedness, emphasizing its alignment with Egypt’s national health security priorities.”
PRET is the system designed to bypass the need for treaty ratification by embedding WHO frameworks in national systems through “technical assistance.”
Once PRET is integrated, WHO gains operational influence during any declared emergency.
Naming PRET outright signals that Egypt’s infrastructure is now being shaped to meet PRET’s requirements for sustained respiratory surveillance and rapid WHO-driven response.
Bottom Line
Egypt’s new WHO-guided influenza and respiratory surveillance upgrade is a quiet rollout of PRET—a framework that centralizes global respiratory monitoring under WHO standards and feeds constant influenza, COVID, bird flu, MERS, and zoonotic signals into real-time digital dashboards.
This turns “preparedness” into a perpetual surveillance regime, where respiratory data becomes the trigger for future restrictions, emergency declarations, and global coordination.
What makes the timing more concerning is that these surveillance expansions are happening as multiple governments continue engineering avian influenza viruses with pandemic traits—yet none of these programs are being halted.
PRET ensures the monitoring grid is in place before the next laboratory-engineered pathogen emerges.
With 270 surveillance officials trained across 30 sentinel sites, Egypt’s national system is now synced to WHO’s operational architecture.
And this same PRET-aligned model is being replicated country by country, building a global respiratory surveillance system that never powers down.
A newly published PLOS Global Public Health paper confirms that researchers were already running multinational experiments to measure how quickly populations could be moved toward COVID-19 vaccination before any product had been authorized.
The authors state clearly:
“We recruited the respondents in late November 2020… before any [vaccines] were officially approved by a government.”
This places the experiment at a time when the public had no approved vaccine, no final safety data, and no access to Phase 3 trial results.
Yet the study was already testing which institutions—WHO, CDC, Oxford, or the Gates Foundation—were most effective at accelerating public willingness to accept a future vaccine.
The Experiment Focused on Uptake Speed, Not Evidence
The survey’s main outcome variable was not clinical.
It was the speed of compliance:
“Respondents were given five options to express whether and when they would choose to get vaccinated if a vaccine were available at no cost. These options were: ‘Yes, within a month,’ ‘Yes, within 2-3 months,’ ‘Yes, within 4-12 months,’ ‘Yes, after a year,’ and ‘No, never.’”
Those responses were then collapsed into:
“early” (within 3 months)
“middle” (4–12 months)
“late,” which includes “never”
The paper describes vaccine hesitancy entirely in terms of “delay”:
“WHO endorsements, alongside the three other public health organizations examined in this study, are associated with a statistically significant, cross-national reduction in vaccine hesitancy, measured as the delay between vaccine availability and willingness to receive it. Our timing-based measure is a meaningful, yet under-studied, dimension of vaccine uptake that directly speaks to the urgency of public health communication during a pandemic.”
The study did not attempt to measure why individuals might wait for more data or how safety information influences decisions.
Hesitancy was defined only as slowness to accept.
Endorsements Were Randomized to Test Which Authority Moves People Faster
The authors explain that each participant was shown randomized vaccine profiles with or without endorsements from major institutions:
“Our experiment randomly varied exposure to vaccine endorsement information from several prominent global health governance players, including the WHO, the Centers for Disease Control and Prevention (CDC), Oxford University, and the Gates Foundation.”
The goal was to quantify the effect of each authority on changing timing behavior:
“WHO endorsements increase individuals’ willingness to get vaccinated more quickly.”
This design treats institutional influence itself as the variable of interest, not the vaccine.
“[T]rust in scientific authorities, including the WHO, positively correlates with increased public willingness to engage in recommended health practices, such as COVID-19 vaccination and compliance with preventive measures.”
The Paper Acknowledges the Experiment Took Advantage of High Uncertainty
The authors state that their framework relies on the public’s vulnerability during uncertain periods:
“During a novel pandemic, significant uncertainty drives individuals to seek expert guidance on preventive measures such as vaccination.”
The experiment uses that uncertainty to measure which voice is most persuasive.
WHO Was Most Effective When It Spoke Early, Before Other Actors
One of the clearest findings is that WHO’s influence is strongest when it is the first or among the first endorsers:
“The WHO has the greatest impact when it is the first (or among the first) of many organizations to endorse a vaccine.”
And that power drops once other organizations join in:
“[T]he impact of WHO endorsements decreases as additional endorsements from other reputable global health actors emerge.”
The authors explicitly describe this as substitutability, meaning WHO’s influence is higher only when information from other actors is absent.
The Study Also Examined How Endorsements Help Drive Uptake of ‘Low-Quality’ Vaccines
A section of the paper focuses on vaccines with:
50% efficacy,
1-year protection duration,
1 in 10,000 severe side-effect rate,
1 in 30 mild-side-effect rate,
which the authors classify as low-quality vaccines.
The paper states:
“[I]t is crucial to examine the influence of WHO endorsements specifically for lower-quality vaccines, as vaccination intentions for these vaccines are likely to be more sensitive to credible endorsements.”
Their simulation results showed:
“[F]or low-quality vaccines… When people are receptive to WHO endorsements, we observe a distinctly higher vaccination rate over time.”
This shows the study’s purpose was not limited to hypothetical best-case vaccines.
The authors tested how institutional messaging can increase uptake even when vaccine performance is weak.
The Authors Describe Their Work as Global-Level Persuasion Research
Throughout the paper, the focus is on influence, not clinical evaluation:
“This study investigates the influence of World Health Organization (WHO)’s endorsements…”
Endorsements “can accelerate vaccination intentions” and “significantly reduce vaccine hesitancy.”
And the authors frame the absence of evidence as an opportunity:
“During a novel pandemic, significant uncertainty drives individuals to seek expert guidance on preventive measures such as vaccination.”
Rather than studying data quality or risk–benefit communication, the study treats this moment of uncertainty as the condition under which endorsement effects can be most accurately measured.
Conclusion
The record in PLOS Global Public Health shows that researchers in Canada, Japan, and the United States were already measuring which institutions could most effectively accelerate COVID-19 vaccine uptake—for low-quality vaccines—in November 2020, prior to any approved product.
The experiment centered on how quickly people could be influenced to vaccinate, how endorsement messaging changes compliance timing, and how those effects behave under uncertainty or when evaluating lower-quality vaccines.
Every element of the study was built around institutional persuasion.
Not safety, not efficacy, and not informed consent.
When institutions are tested for their ability to speed compliance before safety data even exists, the line between public health guidance and psychological manipulation becomes impossible to ignore.
“Because studies have not ruled out the possibility that infant vaccines cause autism.”
The U.S. Centers for Disease Control and Prevention (CDC) has officially declared that there is no evidence to support the claim that vaccines do not cause autism.
Yesterday, the CDC published these historic words:
The claim “vaccines do not cause autism” is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.
The claim “vaccines do not cause autism” is not an evidence-based claim because studies have not ruled out the possibility that infant vaccines cause autism.
HHS has launched a comprehensive assessment of the causes of autism, including investigations on plausible biologic mechanisms and potential causal links.
In an instance of welcome self-reflection and honesty, the CDC announcement went on to admit that the unscientific claim “has historically been disseminated by the CDC and other federal health agencies within HHS to prevent vaccine hesitancy.”
And in an apparent course correction, CDC announced that “HHS has launched a comprehensive assessment of the causes of autism.”
This will include “investigations on plausible biologic mechanisms and potential causal links.”
CDC went on to explain how the rise in autism correlates with the rise in the number of childhood vaccinations:
It is critical to address questions the American people have about the cause of autism to ensure public health guidance is adequately responsive to their concerns. Approximately one in two surveyed parents of autistic children believe vaccines played a role in their child’s autism, often pointing to the vaccines their child received in the first six months of life (Diphtheria, tetanus, pertussis (DTaP), Hepatitis B (HepB), Haemophilus influenzae type B (Hib), Poliovirus, inactivated (IPV), and Pneumococcal conjugate (PCV)) and one given at or after the first year of life (Measles, mumps, rubella (MMR)). This connection has not been properly and thoroughly studied by the scientific community.
In 1986, the CDC’s childhood immunization schedule for infants (≤ 1 year of age) recommended five total doses of vaccines: two oral doses of oral polio vaccine (OPV) and three injected doses of Diphtheria and Tetanus Toxoids and Pertussis Vaccine (DTP). In 2025, the CDC schedule recommended three oral doses of Rotavirus (RV) and three injected doses each of HepB, DTaP, Hib, PCV, and IPV by six months of age, two injected doses of Influenza (IIV) by 7 months of age, and injected doses of Hib, PCV, MMR, Varicella (VAR), and Hepatitis A (HepA) at 12 months of age.
The rise in autism prevalence since the 1980s correlates with the rise in the number of vaccines given to infants. Though the cause of autism is likely to be multi-factorial, the scientific foundation to rule out one potential contributor entirely has not been established. For example, one study found that aluminum adjuvants in vaccines had the highest statistical correlation with the rise in autism prevalence among numerous suspected environmental causes. Correlation does not prove causation, but it does merit further study.
HHS is now researching plausible biological mechanisms between vaccines and autism.
HHS will evaluate plausible biologic mechanisms between early childhood vaccinations and autism. Mechanisms for further investigation include the impacts of aluminum adjuvants, risks for certain children with mitochondrial disorders, harms of neuroinflammation, and more.
CDC provided a chart showing that across three decades of U.S. government reviews, federal agencies (IOM and AHRQ/HHS) have repeatedly concluded that the evidence is insufficient to confirm or rule out a causal link between DTaP/DTP/Tdap/Td vaccines and autism.
The CDC’s newfound scientific approach to autism’s link to vaccines comes after a large McCullough Foundation meta-analysis of 136 studies concluded that childhood vaccination—especially cumulative, clustered, and early-timed dosing—is the strongest modifiable risk factor for autism and other neurodevelopmental disorders.
After decades of denial, the CDC under the Trump administration and HHS Secretary Robert F. Kennedy Jr. has finally taken the first responsible step toward scientific honesty by admitting that vaccines have never been definitively ruled out as a cause of autism.
This is perhaps the strongest decision the agency has made in years.
By abandoning the unscientific slogan and acknowledging the unanswered questions, the CDC has opened the door to the kind of rigorous investigation that should have been undertaken long ago.
For the first time, federal health authorities are conceding that parents’ concerns are legitimate, that autism’s rise demands real answers, and that the expanding vaccine schedule must be scrutinized—not protected.
If the agency continues down this path, the CDC may finally reclaim what it has lacked for a generation: credibility.
We look forward to the CDC being equally honest about COVID-19 vaccines.
Two synthetic H7N7 hybrids demonstrated silent, high-risk shedding behavior in experimental chickens.
The United Kingdom’s top government virology lab engineered new avian influenza viruses using reverse genetics, according to an October paper in Virology documenting the deliberate construction and experimental infection of chickens with synthetic H7N7 avian influenza variants.
The study findings are revealed as the WHO builds a permanent international system for collecting, storing, and redistributing pathogens under its new Pandemic Agreement.
The work, performed at the Animal and Plant Health Agency (APHA-Weybridge), reconstructed the mutation pathway by which low-pathogenic bird flu transitions into a lethal high-path strain.
The study confirms that government researchers created two genetically engineered influenza viruses, altered at the exact molecular switch responsible for converting mild bird flu into its highly pathogenic form.
The paper—“Infection of point-of-lay hens to assess the sequential events during H7N7 high-pathogenicity avian influenza emergence at a layer premises”—states that APHA scientists generated two recombinant H7N7 viruses through reverse genetics (“RG”):
“Two viable RG rescued recombinant LPAIVs were genetically identical to the isolated H7N7-HPAIV except for the CS, with one containing a DBCS (H7N7-DBCS) and the other a SBCS (H7N7-SBCS).”
These engineered viruses were then used to infect groups of live hens under SAPO Level 4/ACDP Level 3 biocontainment—the UK’s highest animal-pathogen security facilities.
The bird flu experiment raises national security concerns, given that Congress, the White House, the Department of Energy, the FBI, the CIA, and Germany’s Federal Intelligence Service (BND) have confirmed that the COVID-19 pandemic was likely the result of lab-engineered pathogen manipulation.
Governments all over the world are performing the same experiments on bird flu pathogens.
Creating New Bird Flu Viruses With Engineered Cleavage Sites
The engineered viruses differed only at the hemagglutinin (HA) cleavage site, the key molecular feature that determines whether an avian influenza virus remains low-pathogenic or becomes systemically lethal.
H7N7-SBCS: a synthetic virus with a single-basic cleavage site
H7N7-DBCS: a synthetic virus with a di-basic cleavage site
Both constructs kept all internal genes identical to a known high-path H7N7 outbreak strain, meaning APHA researchers produced low-path versions of a high-path virus with engineered cleavage-site mutations.
The paper states:
“The SBCS, DBCS and MBCS (HPAIV) viruses were otherwise genetically identical (including the internal genes).”
In plain terms, they took the genome of a highly pathogenic bird flu virus, edited the cleavage site to make it “low-path,” and then infected chickens to observe how the high-path virus might emerge again.
This is the same cleavage-site mutation that historically turns H5 and H7 viruses into lethal strains.
The Engineered Viruses Showed New Functional Behavior
Although created as “low-path” models, the engineered viruses demonstrated new and concerning biological behavior:
Infection rates differed sharply between the constructs.
The DBCS-engineered virus behaved more like a high-path precursor.
Birds exposed to engineered strains survived later high-path challenge—but 95% still shed high-path virus, creating silent spreaders.
The study reports:
“Prior H7N7-LPAIV exposure did not prevent H7N7-HPAIV replication… 20/21 (95%) shed H7N7-HP.”
That means infected birds carried and expelled high-path virus without dying, a dangerous epidemiological function not typical of standard high-path bird flu outbreaks.
This creates a superspreading scenario in which visibly healthy birds shed lethal virus into water, bedding, and surrounding environments.
The environmental sampling confirmed this:
“H7N7-HPAIV environmental contamination occurred… in drinking water and mixed straw/feces.”
A Step-by-Step Reconstruction of How High-Path Bird Flu Emerges
The study explicitly aimed to recreate the sequential mutation steps under which a low-path strain turns into a high-path one.
The authors describe the goal:
“Our current study aimed to model the sequential events… beginning with H7N7-LPAIV incursion, followed 2 weeks later by H7N7-HPAIV challenge.”
This experiment reproduces, in controlled conditions:
Introduction of engineered low-path virus
Mild, low-level infection
A second exposure to a high-path strain
Silent onward shedding of the high-path virus
Environmental contamination
Survival of spreading hosts
This combination of enhanced survival + sustained shedding is precisely the kind of phenotype that raises dual-use questions in influenza engineering.
Conducted in Government BSL-3/4 Facilities
All work occurred at APHA-Weybridge under strict containment:
“Experiments were carried out in UK approved SAPO level 4, ACDP level 3 biocontainment laboratories.”
SAPO Level 4 is one of the highest pathogen-containment designations in the UK, typically associated with agents capable of major agricultural or economic harm.
Bottom Line
A UK government virology lab:
engineered two new influenza viruses,
from a known high-pathogenic backbone,
altered the cleavage site, the genetic switch controlling lethality,
infected live hens with the engineered constructs,
and documented how these modifications enabled silent high-path virus replication and shedding.
This work confirms the intentional creation of new influenza viruses and demonstrates functional behaviors—particularly prolonged shedding without mortality—that raise significant dual-use and biosecurity concerns.
The world may be one step closer to another lab-made pandemic.
The WHO’s new annex would establish a worldwide system for collecting, sharing, and redistributing pathogens—giving the agency a permanent role in directing future pandemic responses.
The World Health Organization (WHO) just took one of its most consequential steps toward centralized pandemic coordination, as governments around the world lab-engineer multiple chimeric bird flu viruses, the very pathogen the mainstream predicts will cause the next pandemic.
In a new announcement from Geneva published on Friday, the agency confirmed that countries are negotiating the first draft of the ‘Pathogen Access and Benefit-Sharing’ (PABS) annex.
This is a legally binding add-on to the WHO’s forthcoming ‘Pandemic Agreement’ that would create a permanent international mechanism for collecting, storing, and redistributing pathogen samples and genetic sequence data.
Across the short press release, the WHO used the word “pandemic” fourteen times, revealing the core justification for what it’s really building: a standing international command network for future pandemic response.
“Countries must be able to quickly identify pathogens that have pandemic potential and share their genetic information and material so scientists can develop tools like tests, treatments, and vaccines,” the WHO said.
A Permanent Infrastructure for Pandemic Coordination
The PABS annex operationalizes Article 12 of the Pandemic Agreement, transforming what was once voluntary information-sharing into a formal, legally binding system.
If adopted, countries will be required to submit both biological materials and genetic data on “pathogens with pandemic potential” into a WHO-coordinated system, effectively creating a multinational pathogen clearinghouse.
In return, the WHO promises “fair and equitable” access to the medical products developed from these materials.
But that access would be managed through the same centralized network, making the WHO not just an advisor, but a logistical coordinator for the entire chain of pandemic response: detection, data, research, and distribution.
‘Solidarity’ as the Framework for Centralized Control
WHO Director-General Tedros Adhanom Ghebreyesus called the move a victory for unity.
“Solidarity is our best immunity,” Tedros said. “Finalizing the Pandemic Agreement, through a commitment to multilateral action, is our collective promise to protect humanity.”
That message of solidarity sounds benevolent.
But in practice, it marks the institutionalization of transnational pandemic management under WHO authority, giving the agency standing powers to organize and direct the movement of pathogen data worldwide.
Risks of an International Pathogen Network
Centralized pathogen-sharing regime raises major risks:
Loss of Sovereignty: Countries could be legally obligated to transfer biological samples and genetic information to the WHO, diminishing national control over biosecurity.
Intellectual Property Exploitation: Data shared through the WHO may be commercialized by corporate or academic partners with no guaranteed benefit to source nations.
Security and Dual-Use Concerns: Centralized pathogen databases become high-value targets for theft or misuse.
Administrative Bottlenecks: Complex “benefit-sharing” rules could delay rapid response—the opposite of what’s promised.
From Agreement to Enforcement
The Intergovernmental Working Group (IGWG) met November 3–7 in Geneva to negotiate the annex, with co-chairs Ambassador Tovar da Silva Nunes (Brazil) and Matthew Harpur (UK) promising a finalized version for adoption at the 79th World Health Assembly in May 2026.
Once approved, national parliaments would begin ratifying the full Pandemic Agreement, paving the way for a unified international system of pathogen control and pandemic coordination.
All anchored in Geneva and legally binding across WHO member states.
Bottom Line
The WHO’s new PABS annex is more than a technical policy.
It’s the foundation of a permanent international pandemic infrastructure, one that centralizes biological data, pathogen access, and emergency response authority under the world’s largest unelected health agency.
Under the banner of “pandemic preparedness,” the WHO is building the system that will coordinate—and possibly control—the next worldwide outbreak response.
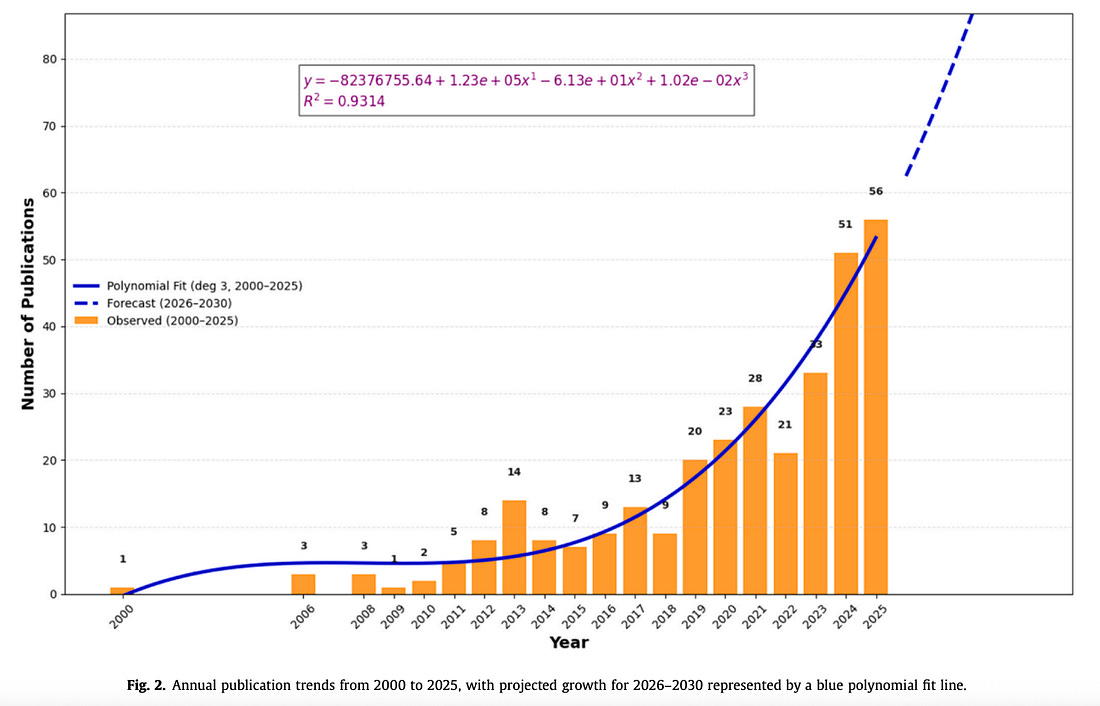
Bird flu publications skyrocket from fewer than 10 papers a year before 2010 to over 50 in 2025—with output expected to hit 111 by 2030, a tenfold surge.
A new Journal of Infection and Public Health paper published this month by Indian Council of Medical Research (ICMR) scientists reveals an unprecedented rise in bird flu–related research worldwide—and predicts that publications on avian influenza will nearly double by 2030, marking what the authors call “accelerating growth” in the field.
The data show that bird flu research output has exploded from fewer than 10 papers a year before 2010 to over 50 in 2025, with the authors projecting a jump to 111 by 2030—a tenfold surge in just two decades, signaling that bird flu has quietly become one of the fastest-expanding areas of global pathogen research.
The figures are based on data from Scopus, a global scientific database that includes most journals indexed in PubMed but extends far beyond biomedical research to cover environmental, veterinary, and policy studies.
This makes Scopus the broadest available measure of the worldwide surge in bird flu–related publications.
The revelation comes as this website has, for years, been raising alarms over the quiet expansion of international bird flu experiments and bird flu pandemic response infrastructure.
The new study, titled “Avian Influenza Research Through the Lens of One Health: A Bibliometric Study” (Elsevier, 2025), analyzed 315 publications on avian influenza between 2000 and 2025 and found that research has exploded since 2018.
The authors expect the trend to continue exponentially over the next five years.
Using a third-degree polynomial model, the team projected that the number of publications will grow from 62 in 2026 to 111 by 2030, with an R² of 0.93 indicating a strong upward trajectory.
“A marked increase occurred after 2018… Forecasts suggest continued growth, with the number of publications expected to rise from 62 in 2026 to 111 in 2030, reflecting increasing research interest and recognition” the paper reads.
The Post-2018 Acceleration
The new study identifies 2018 as the tipping point when H5N1 and One Health publications began to surge.
That timeline aligns with several key developments:
The 2018–2019 launch of the WHO–FAO–OIE–UN pandemic coordination framework under “One Health.”
The rollout of avian influenza vaccination programs in China, which reshaped global research priorities.
The resurgence of EcoHealth Alliance’s field work and U.S. government contracts related to avian flu viruses.
By 2025, the publication rate had risen to 56 papers per year—the highest in two decades
WHO, CDC, and EcoHealth at the Center of the Growth
According to the paper’s institutional data, the U.S. Centers for Disease Control and Prevention (CDC) leads the world in bird flu and One Health research output, followed by the World Health Organization (WHO) and EcoHealth Alliance.
EcoHealth is the same organization whose NIH-funded work in Wuhan has been at the center of worldwide controversy over gain-of-function experiments.
Table 1 lists the CDC as having the highest number of publications (13) with 271 citations, followed by the World Health Organization (WHO) (11 publications) and EcoHealth Alliance (8 publications).
In other words, the primary institutions steering the One Health–avian influenza research ecosystem are the same ones historically involved in dual-use virology, pandemic simulation, and cross-species virus manipulation projects.
‘Enhanced Cross-Sectoral Collaboration’—A Code for Expansion
The authors conclude by urging the global scientific community to strengthen “cross-sectoral collaboration” and “sustained surveillance” in poultry and wild birds, warning against “undetected transmission chains in resource-limited settings.”
While framed as disease prevention, this language mirrors the same pandemic-preparedness justification that has fueled massive funding surges into high-containment labs (BSL-2 and BSL-3) and pathogen collection networks around the world.
The study’s repeated emphasis on “biosecurity,” “interdisciplinary cooperation,” and One Health “integration” signals that governments and international bodies are institutionalizing H5N1 work as a standing global priority, not a short-term emergency response.
Normalizing a Permanent Bird Flu Research Pipeline
The study’s authors celebrate this acceleration as a sign of “increasing research interest and recognition.”
But for many observers, it represents something far more concerning—the normalization of a permanent, internationally coordinated pandemic creation and response regime built around H5N1 bird flu.
The report openly ties its findings to global governance structures such as the WHO and the United Nations, stating that the One Health framework is essential for “multisectoral collaboration” and for guiding “policy and research agendas” on avian influenza.
In effect, the paper documents the institutionalization of bird flu research as a permanent fixture of global biosecurity policy—a shift that blurs the line between public health and biodefense, and raises serious questions about how far these programs will go.
Bottom Line
The new Journal of Infection and Public Health study confirms what many have suspected: since 2018, there has been a coordinated expansion of avian influenza research worldwide.
WHO, CDC, and EcoHealth Alliance are leading the charge, and the scientific community now projects that output to double by 2030.
Behind the rhetoric of “One Health” and “collaboration” lies a long-term global infrastructure for studying, modifying, and surveilling avian viruses — one that could easily serve both pandemic prevention and pandemic creation agendas.
The normalization of this permanent H5N1 research pipeline marks the next chapter in the international “pandemic preparedness” agenda — and the public deserves to understand what’s being built, and why.
The claim is simple. When the U.S.-linked market access to security performance, Mexico moved against the cartels with a speed and scale that years of soft talk never achieved. The point is not that tariffs alone solve organized crime. The point is causal leverage. When the largest customer in North America threatened to price Mexico’s exports out of its own market, Mexico recalibrated. When the U.S. paired that leverage with focused intelligence sharing, extraditions, and sanctions, cartel decision makers faced new constraints. The cartel economy depends on cross border flows, logistics corridors, and financial rails that are sensitive to bilateral friction. Diplomatic pleasantries never touched those levers. Tariff brinkmanship did, and it did so without a shot fired across the border.
Skeptics will say that economics cannot beat criminal networks. That claim confuses the target. The goal is not to reform the soul of a cartel. The goal is to force political actors in Mexico to prioritize enforcement against violent groups, to permit deeper cooperation with U.S. agencies, and to accept the reputational and domestic risks that come with taking on entrenched mafias. Mexico takes those risks only when the alternative is costlier. Tariff threats change that calculus overnight. They reprice inaction in clear numbers, jobs at risk, plants at risk, export earnings at risk. Ministries respond. Governors respond. The National Guard deploys. Judges sign extraditions they once delayed. That is what happened when tariffs entered the conversation, first in 2019, then again in Trump’s second term. Today that proven leverage is under attack in courtrooms, where Democrat-led lawsuits seek to strip the president of the authority to use tariffs as a national security tool. If those suits succeed, they will not restrain Trump, they will embolden the cartels and every foreign adversary that profits from American weakness.
To see the mechanism, begin on the ground in western Mexico. In regions of Jalisco, Colima, and Michoacán, the Jalisco New Generation Cartel operates like a parallel government. It taxes businesses, regulates who may operate on its turf, and even puts its name on public fiestas. In one municipality, banners thanked Nemesio Oseguera, known as El Mencho, for sponsoring gifts for children. In another, locals used a cartel built clinic in Villa Purificación because state services were absent. None of this is surprising in weak state zones. What matters for U.S. policy is that these enclaves sit astride the logistics spine that feeds the U.S. market. Ports like Manzanillo move containers from South America and Asia. Highways north carry drugs, migrants, and money. If U.S. trade policy threatens those arteries, Mexico City has incentives to restore the state’s writ in the corridors that matter most.
El Mencho’s organization is not a local street gang. It fields a layered security apparatus, including a special unit equipped with rockets and grenades. In 2015, CJNG gunmen shot down a Mexican military helicopter during an operation, a shocking display of firepower that advertised the cartel’s confidence. The group also ring fences mountain strongholds with scouts, roadblocks, and mines. Raids provoke citywide arsons and road closures in Guadalajara and into Guanajuato. In such a setting, hand wringing about social programs sounds detached. What shifts behavior is when Mexico’s leaders face a macroeconomic penalty for letting these fiefdoms endure. Tariff leverage reaches that level, and the evidence shows it can set in motion the interagency machinery that hits labs, financiers, and mid level operators at volume.
Consider the drug market context. Coca production in the Andes has surged, which flooded the wholesale market with cheaper product. Cocaine moved back to center stage after several years of fentanyl headlines. A group like CJNG, with strong Pacific port access and partnerships in Colombia, could ride that wave and offset pressure on synthetics. Meanwhile, the Sinaloa Cartel leaned heavily into fentanyl and faced increasing U.S. targeting of precursors and labs. The U.S. pressed China on precursor exports, tightened seizures, and pushed Mexico to raid fentanyl processing sites. That pressure reduced margins on synthetics and raised risk. Paired with tariff leverage, it created a squeeze that encouraged Mexico to help dismantle labs and disrupt supply hubs. Markets matter. Enforcement that changes marginal profit and risk in the short run redirects cartel effort. The United States cannot erase demand, but it can force suppliers to operate under costly uncertainty.
The 2019 episode is instructive. When the administration threatened across the board duties, Mexico agreed to deploy its newly formed National Guard along migrant and contraband routes and to accept additional enforcement commitments. Analysts can debate the migration details, but the security effect is clear. Mexico acted quickly because the cost of not acting would fall on sectors that anchor the country’s growth. That logic returned in 2025 when the administration raised the prospect of tariffs again, this time coupled to anti cartel benchmarks. The message to Mexico’s leadership was consistent. Move against the cartels, deepen intelligence cooperation, accelerate extraditions, or face economic pain. The result was concrete. Mexico intensified joint work with U.S. agencies, stood up mixed intelligence cells, and green lit mass transfers of suspects to face U.S. charges. In two waves, more than fifty alleged traffickers were expelled to the United States, a scale of cooperation that older, dialogue heavy frameworks never achieved.
Critics will ask, is this sustainable, or does it merely export violence from one plaza to another. The answer is that sustainability depends on continued leverage and on aligning incentives for Mexican elites. Tariff pressure does not replace police reform or judicial independence. It does not remove human rights obligations. It does force short term action that changes cartel cost structures and supply chain reliability. Those changes shift the balance of power among criminal groups in ways that can be exploited by further policy. For example, when the Sinaloa Cartel fractured between Los Chapitos and the Mayo faction, concentrated pressure on fentanyl labs and logistics widened fissures. Leadership arrests and extraditions reduced the ability to mediate disputes. Reports of improvised alliances with CJNG in select corridors show how stress from enforcement can bend even bitter rivals toward short term deals. This is not a reason to stop. It is an opening to target the new vulnerabilities that arise when groups are on the back foot.
A common objection says that tariffs punish lawful commerce and could harm North American supply chains. That is true in the abstract, and it is exactly why they work as leverage rather than as a permanent policy. The aim is not to collect tariff revenue. The aim is to condition zero tariffs on measurable security cooperation. Think of it as a switch rather than a steady tax. The threat must be credible, and the off ramp must be clear. Mexico is a sophisticated exporter with deep stakes in the U.S. market. The possibility of losing preferred access focuses the mind in ways that speeches do not. When the policy is paired with clear asks, like named extraditions, joint targeting packages, and verified lab demolitions, the switch can be flipped off once outcomes appear. That is what distinguishes hard power diplomacy from appeasement. Appeasement sends signals of patience. Tariff leverage sends deadlines.
Another objection says that designating cartels for terrorism related authorities escalates needlessly. Here the right comparison tool is cost benefit analysis grounded in law. Transnational criminal groups that use mass intimidation, car bombs, and targeted assassinations are already functionally political actors in their domains. Terror designations and global terrorist sanctions unlock financial and legal tools that undercut safe haven logistics, donor networks, and procurement. The January 2025 executive order that directed the application of terrorism authorities against cartels and their enablers had predictable effects. Banks expanded de risking around suspect nodes. Shell entities tied to weapons procurement felt pressure. Partners in the region had clearer legal hooks to cooperate. Mexico’s government will always defend sovereignty in public. In private, those tools make joint operations more effective, and they do so without violating Mexico’s constitution or inviting U.S. troops to patrol Mexican cities.
Evidence of impact is not limited to courtroom dockets. Culture reacts to power. Narco ballads that praise El Mencho surged in popularity after high profile performances, but public backlash mounted when new gravesites and extermination sites were uncovered in Jalisco. U.S. actions that restricted visas for performers who glorified capos caused cancellations that hit one of the propaganda pipelines. Small signals matter when trying to erode the social capital that cartels buy through patronage. Meanwhile, binational operations disrupted prestige capabilities, including the use of drones, ultralights, and submersibles. Interdictions on the Pacific and seizures at U.S. ports cost real money. Every delay reduces throughput and degrades customer trust. Importantly, as the U.S. targeted financial nodes, cryptocurrency laundering schemes lost channels, and front businesses faced pressure, which raised the price of moving funds covertly.
To be sure, CJNG has proved adaptive. Its decentralized network of regional cells, each with autonomy in local rackets, gives it resilience. Franchising tactics allow the brand to expand without a single point of failure, and harsh internal discipline suppresses splintering. A top down foe like Sinaloa has suffered succession crises, especially after leadership arrests and extraditions. That difference, however, strengthens the case for tariff leverage rather than weakens it. Decentralized cartels thrive in the gaps created by half measures. They are less sensitive to symbolic arrests. They are more sensitive to systemic friction on the trade and logistics platforms that run through their territories. When Mexico clears the roadblocks, literally and figuratively, to keep trade and investment flowing, it also clears a path for the state to reassert control in strategic corridors. The federal government does not need to pacify every mountain village at once. It needs to squeeze the chokepoints that matter for commerce. Tariff threats direct political energy toward those chokepoints.
What about the demand side in the U.S. Demand for stimulants and opioids remains the engine, and it would be naive to claim that supply side tools alone will solve addiction. That point is compatible with the tariff argument. The claim here is modest. Among available foreign policy levers, tariff backed conditionality plus intelligence pressure delivers more enforcement cooperation from Mexico than legacy dialogues and diplomatic communiqués. When used episodically and with precision, tariff threats avoid long term harm to North American competitiveness while achieving short term security gains that no other tool has produced. In the language of philosophy, this is a comparative institutional claim. Competing institutions, like multiyear dialogue frameworks or aid packages, have failed to generate sustained Mexican action commensurate with the threat. Tariff leverage has.
The comparison with appeasement is direct. For decades, U.S. officials accepted assurances without benchmarks, and they treated cartel control as a domestic Mexican issue. That posture delivered cartel rule in multiple municipalities, a surge in public displays of brutality, and brazen attacks on state assets. The 2015 helicopter shoot down marked a threshold. After that, the claim that cartels could be managed with business as usual was no longer credible. The years that followed saw waves of violence in Culiacán and beyond as factions inside Sinaloa fought, while CJNG spread by absorbing orphaned cells and imposing its own savage order. It is only when credible economic sanctions entered the equation that Mexico’s federal government matched words with deeds at scale. That is not a moral judgment about Mexico. It is a structural observation about incentives in an integrated market.
Looking ahead, the template is clear. Maintain the credible threat of tariffs tied to verifiable security actions. Deepen joint intelligence cells in Mexico City and Monterrey. Use terrorism designations and global terrorist sanctions to freeze assets, restrict travel, and criminalize material support networks. Prioritize extraditions of logisticians, financiers, chemists, and weapons brokers, not just marquee capos. Leverage public diplomacy to delegitimize narco culture while supporting civil society in affected towns. Reward compliance quickly by suspending tariff threats once targets are met. Reimpose pressure if backsliding occurs. That is a strategy that respects Mexican sovereignty, because it offers choices, yet it also respects American lives, because it insists on measurable outcomes.
The hard question is whether Mexico will cooperate without the tariff lever. The evidence suggests not. Governments everywhere respond most reliably to concrete costs and benefits, not to abstract pleas. The U.S. should not apologize for using its market access to defend its citizens from poisoned drugs and cross border violence. Nor should it romanticize soft power that has failed in the face of organizations that rule by fear. Cartels that behave like insurgent states invite a policy that treats them as such, within law, with calibrated coercion, and with clear diplomatic exits. Trump’s doctrine did that. It made the cartels and their protectors blink. That proven leverage is now under attack in courtrooms, where Democrat-led lawsuits seek to strip the president of the authority to use tariffs as a national security tool. If those suits succeed, they will not restrain Trump—they will embolden the cartels and every foreign adversary that profits from American weakness. That is progress measured in extradition receipts, dismantled labs, interrupted shipments, and smaller propaganda stages for the narco balladeers. It is not the end of the problem, but it is the first policy in years that has shifted the equilibrium in the right direction.
Internal NETEC document confirms H5N1 avian influenza preparedness at the core mission of new taxpayer funded hospital network.
The U.S. Department of Health and Human Services (HHS), through its Administration for Strategic Preparedness and Response (ASPR), is funding a $37.5 million national hospital expansion to prepare for H5N1 bird flu and other high-consequence pathogens, according to a newly released internal federal document issued by the National Emerging Special Pathogens Training and Education Center (NETEC).
NIH and NIAID—which are under HHS, led by Secretary Robert F. Kennedy Jr.—are funding experiments that create brand new bird flu pathogens, raising conflict of interest worries as well as questions about the government’s motives (see list of articles below this article detailing these many experiments).
The new document—an internal Request for Proposal (RFP) dated October 15, 2025—details how HHS will use NETEC, a consortium of Emory University, the University of Nebraska Medical Center, and NYC Health + Hospitals/Bellevue, to distribute federal funds to 75 hospitals across the United States, converting them into federally designated “Level 2 Special Pathogen Treatment Centers” (SPTCs).
The RFP’s stated purpose is to “accelerate the domestic health care system’s readiness for [high-consequence infectious diseases], such as H5N1, Ebola, and others.”
Per the document:
“Under the guidance of ASPR, NETEC is now awarding $37,500,000 in funding to 75 facilities ($500,000 per facility) as they work to meet the requirements of NSPS Level 2 facilities. The funding will support activities such as training health care personnel, upgrading infrastructure, and acquiring specialized equipment to ensure Level 2 facilities meet NSPS minimum capabilities. These efforts are expected to ultimately result in the verification of funded facilities as Level 2 SPTCs. This expansion significantly enhances the nation’s surge capacity and geographic reach for managing HCIDs.”
The move comes as governments all over the world say they are creating hybrid bird flu viruses in biolabs, raising national security fears of another pandemic, whether intentional or accidental.
Those same countries ramp up bird flu vaccine production and distribution.
Meaning, once again, governments are creating both the problem and “solution” to another pandemic, raising conflict-of-interest worries.
H5N1 Avian Influenza Explicitly Listed as a Federal Priority
While the public press release announcing the grant avoided mentioning bird flu, the internal NETEC RFP directly names H5N1 avian influenza as a top threat driving the new hospital buildout.
“The emergence and sustained transmission of HCIDs, such as Ebola, mpox, and avian influenza (H5N1), have overwhelmed hospitals, exhausted critical resources, and underscored the necessity for coordinated efforts to protect health care workers while ensuring the delivery of safe and effective patient care.”
This wording makes clear that H5N1 preparedness—not just general infectious disease readiness—is a central justification for the $37.5 million initiative.
Federal Pandemic Infrastructure Expansion
Under ASPR’s direction, NETEC will administer the new program as part of the National Special Pathogen System (NSPS)—a tiered national network of pathogen treatment centers first created after the 2014–2016 Ebola outbreak.
The new Level 2 centers are described as “the backbone of a resilient, skilled response to special pathogen threats,” designed to serve as regional treatment hubs capable of handling clusters of patients during future high-consequence disease outbreaks.
The funding will support:
Upgrading isolation infrastructure,
Purchasing specialized containment equipment,
Training staff in special pathogen protocols, and
Coordinating with existing Level 1 Regional Emerging Special Pathogen Treatment Centers (RESPTCs).
Awardees must demonstrate “substantial progress towards meeting the minimum capabilities of a Level 2 NSPS facility” by the end of the funding period.
‘Level 2’ Centers Will Treat Patients for the Duration of Illness
Each Level 2 facility, the RFP explains, must have “the capacity to deliver specialized care to clusters of patients suspected of or infected by a special pathogen” and “serve as the primary patient care delivery center.”
Notably, funded hospitals must also agree to:
“Serve as regional and national assets and accept patients from outside of the United States or outside their respective state, county, or local jurisdiction if requested.”
That clause effectively integrates participating hospitals into the federal pandemic command structure under ASPR oversight, expanding the U.S. government’s ability to move special pathogen cases across state or national lines.
Institutionalization of Permanent Biosecurity Infrastructure
The NETEC RFP uses unmistakable national security language, describing high-consequence infectious diseases (HCIDs) as threats to “the nation’s health, economy, and national security.”
It emphasizes what it characterizes as the need for “enhanced biosecurity frameworks, robust clinical readiness, and surge capacity across hospitals,” positioning the Level 2 expansion as a cornerstone of HHS’s long-term pandemic preparedness architecture.
The RFP even notes that NETEC “has demonstrated its critical role in strengthening national health security by coordinating National Special Pathogen System responses to novel respiratory pathogens, mpox, and Lassa fever.”
In other words, the federal government is now formally embedding outbreak containment systems inside civilian hospitals, justified by avian influenza and other potential zoonotic spillover threats.
Timeline & Implementation
Applications for the NSPS Level 2 STAND Award opened October 15, 2025, and close December 2, 2025.
Final selections are expected by January 5, 2026, with the official “period of performance” scheduled from January 5 through June 29, 2026.
Eligible applicants must have:
An onsite emergency department,
Airborne infection isolation rooms,
Critical care and inpatient capacity, and
A sufficient baseline of resources to achieve Level 2 verification.
The RFP explicitly prohibits use of the funds for direct clinical care or research—focusing instead on infrastructure, staff training, and equipment acquisition.
From COVID Lessons to Bird Flu Systems
NETEC was originally established in 2015 after the U.S. treated imported Ebola cases.
During the COVID-19 pandemic, it served as a national training and coordination body for pathogen response across hospitals.
Now, under ASPR’s expanded authority, NETEC’s mission has evolved from temporary outbreak response to permanent pandemic infrastructure building, with H5N1 preparedness front and center.
The RFP states that the expansion “significantly enhances the nation’s surge capacity and geographic reach for managing HCIDs,” embedding what amounts to federally funded containment capacity across the entire U.S. hospital network.
Bottom Line
The internal NETEC document reveals that HHS’s Administration for Strategic Preparedness and Response (ASPR) is quietly constructing a nationwide bird flu hospital network under the banner of “special pathogen preparedness.”
The $37.5 million program explicitly cites H5N1 avian influenza as a primary threat and converts 75 hospitals into federally integrated treatment hubs for future high-risk pathogen outbreaks.
This marks yet another major escalation in the institutionalization of permanent pandemic infrastructure inside the United States, built through administrative expansion under the HHS biosecurity apparatus.


























Recent Comments