All participants had already received prior COVID vaccinations, making it impossible to determine whether observed immunity came from the experimental shot, prior vaccines, or natural infection.
Researchers behind an experimental AI-designed “pan-Sarbecovirus” COVID vaccine recorded 148 separate adverse events among just 39 vaccinated participants during a first-in-human clinical trial published last month in the Journal of Infection.
The vaccine, known as pEVAC-PS, was developed using “Digitally Immune Optimised Synthetic Vaccine” (DIOSynVax) technology and was computationally engineered to target not only SARS-CoV-2, but a broad family of purportedly related bat coronaviruses.
The vaccine was delivered through a needle-free intradermal injection system using the PharmaJet Tropis device.
The mainstream is celebrating the drug as a “world-first.”
However, according to the paper, researchers documented:
121 unsolicited adverse events,
15 adverse events of special interest (AESIs),
and 12 clinically significant laboratory adverse events
across only 39 vaccinated participants.
That’s roughly 3.8 total recorded adverse-event entries per vaccinated participant in the small phase I trial.
The study further states that 23 of the unsolicited adverse events were considered “possibly,” “probably,” or “definitely” related to the vaccine.
The paper nevertheless repeatedly describes the vaccine as “well tolerated.”
The paper downplays the severity of the adverse events, but the raw numbers remain notable relative to the tiny sample size—especially given the vaccine failed to demonstrate broad or robust neutralizing activity.
“No serious adverse reactions (SARs), suspected unexpected adverse reactions (SUSARs) or serious adverse events (SAEs) occurred. There were 15 adverse events of special interest, all of which were COVID-19 episodes which were of grade one or two severity and did not require medical attention. There were 121 unsolicited adverse events, all of which were grade one or two severity and 23 were deemed possibly, probably or definitely related to the vaccine. There were 12 laboratory adverse events considered clinically significant, all of which were grade one or two severity and self-resolved without intervention during the study.”
“All four dose concentrations of pEVAC-PS were generally well tolerated.”
Adverse-event burden is being generated in a trial so small that even a modest number of reactions changes the overall safety picture.
The authors do not provide a detailed breakdown of the specific unsolicited adverse events, raising questions about whether the paper’s reassuring “well tolerated” framing would hold up under full public disclosure of the actual reactions recorded during the trial.
Without a transparent symptom-by-symptom breakdown, readers are largely being asked to accept the authors’ safety characterization at face value.
Vaccinated Received Previous COVID Shots, Making Cause of Immunity Impossible to Determine
The trial was conducted between December 2021 and September 2023 and involved healthy adults between ages 18 and 50 who had already received two or three prior COVID-19 vaccine doses.
Since the participants were already heavily pre-immunized before receiving the experimental vaccine, the researchers themselves acknowledge they could not cleanly isolate what immune responses actually came from the new vaccine.
“Interpretation of immunogenicity outcomes was influenced by high baseline antibody levels and heterogeneous exposure histories due to ongoing waves of Omicron variant infections during recruitment, which differed across dose-escalation cohorts and introduced unavoidable immune bias,” the study reads.
The study cannot determine whether any observed immunity came from:
the new AI-designed vaccine,
prior COVID shots,
prior natural infections,
or combinations of all three.
That is why the paper ultimately falls back to cautious language like:
“modest immunogenicity,”
“limited boosting,”
and merely “supporting the underlying design concept” rather than demonstrating clear protective efficacy.
The authors acknowledged the findings did “not support a robust vaccine-induced increase in antibody responses beyond pre-existing levels.”
The paper further admits the vaccine failed to produce the intended broad coronavirus immune-boosting effect:
“Although pEVAC-PS was designed to elicit cross-reactive responses against both SARS-CoV-2 and SARS-CoV-1, this intended boosting effect was not observed.”
Researchers additionally acknowledged the vaccine did not demonstrate “broad or robust neutralizing activity.”
Researchers from the University of Cambridge, University of Southampton, Imperial College London, DIOSynVax Ltd, and other institutions participated in the study.
As the U.S. simultaneously performs similar gain-of-function lab experiments.
Chinese state-backed scientists claim to have engineered multiple mutant H5N1 bird flu viruses and experimentally infected mammals to identify genetic combinations that dramatically increased lethality and enhanced the virus’s compatibility with human cellular machinery, according to a new peer-reviewed paper published yesterday in Emerging Microbes & Infections.
The revelation about China comes as a recent HHS-funded study says that U.S. scientists have also lab-engineered brand-new reassortant “Frankenstein” bird flu viruses with enhanced immune-evasion potential in humans.
The back-to-back disclosures represent an accelerating international effort by government-backed scientists to engineer and characterize bird flu strains with enhanced mammalian adaptation, immune evasion, and pandemic potential.
The creation of pandemic pathogens raises international security and informed consent concerns.
The new Chinese study was conducted at the Harbin Veterinary Research Institute (HVRI), part of the Chinese Academy of Agricultural Sciences (CAAS), using ABSL3 high-containment laboratories approved for work with highly pathogenic avian influenza viruses.
Using an eight-plasmid reverse genetics system, researchers generated reassortant and mutant (“Frankenstein”) H5N1 viruses carrying specific polymerase mutations associated with mammalian adaptation.
The purported engineered viruses were then administered intranasally into BALB/c mice to measure tissue spread, replication efficiency, and lethality.
According to the paper, one engineered strain replicated throughout the body, spreading into the lungs, nasal turbinates, brain, spleen, and kidneys.
Researchers reported that the highly pathogenic strain displayed at least a “560,000-fold” difference in lethality compared to a genetically similar H5N1 virus.
The paper identified three mutations in the PB2 polymerase protein—384L, 443R, and 460M—that together dramatically increased virulence in mammals.
The authors say the mutations allowed the virus to more efficiently exploit human ANP32A/B proteins, which are said to be critical host factors required for influenza replication in human cells under the mainstream virological model.
In plain terms, the researchers are claiming to have identified mutational combinations that helped bird flu function more effectively inside human biological systems.
The experiments align with published gain-of-function definitions involving enhanced pathogen lethality, mammalian adaptation, and viral replication in human cellular systems.
According to a 2022 review published in Advances in Applied Microbiology:
“Gain-of-Function research on viruses is enhancing transmissibility, virus replication, virulence, host range, immune evasion or drug and vaccine resistance to get insights into the viral mechanisms, to create and analyze animal models, to accelerate drug and vaccine development and to improve pandemic preparedness.”
The Chinese study qualifies because the researchers engineered mutant H5N1 viruses that became more lethal in mammals while also enhancing the virus’s ability to replicate and adapt inside human cellular systems.
The study was funded by:
China’s National Key Research and Development Program,
the National Natural Science Foundation of China,
the Natural Science Foundation of Heilongjiang Province,
After WHO—also funded by Gates—declares Ebola a “public health emergency of international concern” and calls for vaccine development, raising conflict-of-interest concerns.
The Bill Gates-funded Coalition for Epidemic Preparedness Innovations (CEPI) will “urgently accelerate development of three investigational vaccines targeting the Bundibugyo Ebola virus that has caused a rapidly spreading epidemic in the Democratic Republic of the Congo (DRC) and neighboring Uganda,” according to a Sunday press release from the organization.
The move comes as the World Health Organization (WHO), also funded by Bill Gates, just weeks ago declared Ebola currently represents a “public health emergency of international concern (PHEIC)” and that there is a need to “[i]mplement clinical trials to advance the development and use of candidate therapeutics and vaccine, supported by partners.”
CEPI now believes there is a “critical need to produce tools to help curtail the outbreak, complementing ongoing public health interventions by affected countries.”
The arrangement raises obvious conflict-of-interest concerns, as Bill Gates-funded transnational health organizations are simultaneously framing the outbreak response, declaring international emergency status, and accelerating the development and deployment of the very vaccine platforms their aligned networks support and finance.
The three vaccine candidates include those developed by the International AIDS Vaccine Initiative (IAVI), Moderna, and the University of Oxford.
CEPI has committed $50 million to Moderna (mRNA platform), $8.6 million to the University of Oxford (adenoviral vector platform), and $3.2 million to IAVI (rVSV vaccine platform).
The press release confirms Moderna’s Ebola formulation will be based on mRNA, like its COVID-19 jab:
“CEPI has committed up to US$50 million for preclinical testing and Phase 1 clinical trials. CEPI will support simultaneous manufacturing of doses to enable large-scale Phase 2/3 trials to begin immediately if Phase 1 data supports progression. This candidate uses the same fast, flexible, scalable mRNA technology validated during COVID-19 and builds upon Moderna’s existing R&D on related Ebola viruses. The collaboration leverages CEPI’s existing strategic partnership with Moderna.”
The same Gates-funded global health network shaping international Ebola messaging, emergency declarations, and government outbreak response is also funding and accelerating the vaccines being presented as the solution to the crisis.
The arrangement raises obvious conflict-of-interest concerns, as the organizations influencing public fear, policy, and emergency infrastructure are financially and operationally tied to the very pharmaceutical platforms being advanced in response.
Fort Detrick hantavirus genome manufacturing project operated through HHS/NIAID-linked high-containment biodefense contracts worth up to $387.5 million combined.
May 13, 2026
The published Andes hantavirus genome sequence was built at the infamous U.S. military biolab Fort Detrick from fragmented sequencing reads extracted from human blood using computer assembly software and reference genome fill-ins, according to supplementary appendix documents and GenBank records tied to a 2020 New England Journal of Medicine (NEJM) paper.
The paper’s funding disclosure shows the Fort Detrick hantavirus genome reconstruction work was supported through U.S. government biodefense and infectious disease funding channels tied to HHS/NIAID (HHSN272201800013C and HHSN272200700016I), including contracts involving Battelle Memorial Institute and Laulima Government Solutions.
The total potential funding allocated to the two Fort Detrick/NIAID contracts together is approximately $387.5 million.
The records show scientists at the United States Army Medical Research Institute of Infectious Diseases (USAMRIID) were said to have physically received blood samples from purported hantavirus patients and used those samples to generate the genome sequence now stored in GenBank and cited throughout the scientific literature.
That same Fort Detrick-built Andes hantavirus genome sequence is now being used by researchers as a reference genome for analyzing and comparing sequences tied to the recent 2026 hantavirus outbreak aboard the cruise ship MV Hondius.
The connection raises major questions about whether modern outbreak detection, genomic surveillance, and authoritarian pandemic-response systems are increasingly being built around computer-reconstructed reference sequences generated inside military and biodefense research pipelines rather than directly sequenced purified viral isolates.
If the foundational genome sequences driving PCR testing, outbreak tracking, quarantine policies, surveillance systems, and vaccine development are themselves heavily dependent on computer reconstruction, statistical modeling, and reference-sequence fill-ins rather than direct uninterrupted sequencing of purified viral isolates, it raises profound questions about whether the entire pandemic-response framework is becoming increasingly circular and self-referential.
Which makes the system potentially weaponizable, because whoever controls the reference sequences, computational pipelines, and diagnostic standards effectively controls the foundation upon which outbreaks are detected, modeled, declared, and responded to.
“Whole-blood samples from 28 (82% of 34) laboratory-confirmed cases from the Epuyén ANDV-caused hantavirus pulmonary syndrome outbreak were included in the genomic analysis.”
Researchers further wrote:
“RNA was extracted from 400 µl of whole blood…”
The appendix also says the samples were physically transferred into the Fort Detrick military biodefense system:
“Samples were shipped to USAMRIID under material transfer agreement (MRMC control number: W81XWH-18-0469)…”
Meaning the published hantavirus genome was generated from fragmented RNA sequencing reads extracted directly from mixed human blood samples handled inside a U.S. military biolab pipeline.
Scientists Say They Removed Human Genetic Material Before Building the Genome
The records show Fort Detrick scientists did not directly sequence one complete uninterrupted hantavirus genome from purified viral particles.
Instead, the workflow involved:
extracting mixed genetic material from human blood,
computationally removing human sequences,
assembling fragmented sequencing reads into partial genome pieces called contigs,
and filling missing genomic gaps using previously published reference sequences from GenBank.
The appendix explicitly states:
“Human genome and human transcriptome read removal was subsequently performed by aligning quality-trimmed reads to the human genome reference GRCh38…”
Meaning Fort Detrick scientists claim to have first filtered out human genetic material from the blood-derived sequencing data before assembling the remaining fragments into what became the published Andes hantavirus genome.
But because the original material consisted of mixed human blood-derived sequencing fragments rather than a directly sequenced purified viral isolate, the final published genome still depended on computational interpretation, reconstruction decisions, and reference-guided fill-ins to determine what ultimately counted as the “hantavirus” sequence.
The final published genome was not simply “read” directly from a purified viral particle.
It emerged through multiple layers of computer-driven filtering, reconstruction, statistical consensus calling, and reference-sequence patching performed inside the Fort Detrick bioinformatic pipeline.
The Published Genome Was Patched Together Using Reference Sequences
The appendix explains how the genome was assembled:
“To generate ANDV consensus genomes, cleaned reads were assembled de novo using SPAdes…”
However, the sequencing data did not produce complete uninterrupted genomes directly from patient blood samples.
Instead, researchers acknowledged that missing regions of the genome had to be filled using previously published genome sequences:
“Gaps and ends of incomplete contigs were filled in with sequences from close complete genomic segments from GenBank…”
Meaning portions of the final published hantavirus genome were patched together using older reference genome sequences where direct sequencing data was missing or incomplete.
The appendix additionally states:
“Only bases with a Phred quality score >Q20 and a minimum of 3X coverage were used for consensus calling.”
Consensus calling is a computer process that generates a “best-fit” genome sequence from fragmented sequencing reads after filtering, alignment, and reconstruction.
If parts of the published hantavirus genome were missing and had to be filled in using older reference sequences, then how much of the final genome was directly sequenced from patient blood and how much was computer-generated reconstruction?
Some Genome Segments Were More Than Half Missing
The records further reveal that some genome assemblies were substantially incomplete before reconstruction and reference fill-ins were applied.
Table S3 shows one patient’s L segment achieved only:
“3080/6562 [46.94%]” coverage
Meaning more than half of that genome segment was missing before additional reconstruction and reference-genome fill-ins were used to complete the published sequence.
Other patient samples achieved much higher coverage, with many approaching 99%, but the appendix confirms incomplete contigs and missing genomic regions were a recurring part of the assembly workflow.
This means portions of the published hantavirus genome were not directly sequenced from patient material, but instead were computationally reconstructed and patched together where the original genomic data was missing.
This raises major questions about the precision and reliability of the final published genome, since significant portions of some sequences were missing and later reconstructed through computer-based reference fill-ins rather than directly sequenced from patient material.
PCR Primers Also Matched Human Genetic Material
The significance of the findings becomes even greater when viewed alongside recent BLAST analyses showing that published hantavirus PCR primers and fluorescent probes repeatedly matched human genetic material.
According to the analysis:
“portions of the genetic sequences used by the PCR test to supposedly detect hantavirus also directly match human DNA sequences.”
The report documented repeated:
19/19 exact matches,
20/20 exact matches,
18/18 exact matches,
and numerous 17/17 exact matches between hantavirus PCR components and human genomic regions.
The fluorescent detection probe itself—the component responsible for generating the “positive” PCR signal—also produced repeated exact and near-exact human DNA matches.
The findings become especially significant in light of the Fort Detrick workflow, which itself began with mixed human blood samples and required computational subtraction of human genetic material before the genome was assembled.
The overlap raises obvious questions about how confidently the PCR system could distinguish purported hantavirus genetic material from human genetic material when the published reference genome itself was reconstructed from mixed human blood-derived sequencing data.
DARPA Documents Reveal Pentagon Framework for Digital-Only Viral Sequences
The Fort Detrick hantavirus reconstruction workflow also aligns with previously released DARPA documents describing Pentagon-backed systems designed to operate even when:
“only electronic viral sequence information may be available.”
The DARPA records describe systems designed to:
take digital genome sequences,
synthesize infectious clone genomes,
propagate viruses in cell systems,
and rapidly convert uploaded genetic sequences into mRNA countermeasures.
The platform is meant to work even when no physical virus exists, only a computer file.
The files state:
“Because we recognize the potential that during a pandemic outbreak only electronic viral sequence information may be available…”
GenBank Entry Confirms Human Blood Origin of Hantavirus Genome
The GenBank entry tied to the outbreak independently confirms the biological source material used to generate the published genome.
The entry states:
/isolation_source=“whole blood”
The GenBank metadata also lists the computer assembly pipeline used to generate the genome:
Ray
Bowtie2
Picard
Prinseq-lite
Cutadapt
Illumina sequencing
The NEJM appendix and GenBank records do not describe:
purification of intact viral particles,
plaque isolation,
viral culture purification before sequencing,
or direct sequencing of purified virions.
Instead, the records show the published Andes hantavirus genome was assembled at Fort Detrick from fragmented sequencing reads extracted from human blood after human genetic material was computationally removed and missing genomic regions were filled using previously published reference genome sequences.
Bottom Line
The records show a biodefense and outbreak-response framework increasingly centered around computationally reconstructed genome sequences generated from fragmented mixed biological material and supplemented through reference-guided assembly pipelines rather than direct uninterrupted sequencing of purified viral particles.
Those computer-assembled consensus genomes then become the foundation for:
PCR testing,
phylogenetic modeling,
transmission mapping,
reproductive-number calculations,
outbreak tracking,
quarantine policies,
surveillance systems,
and vaccine or mRNA countermeasure development.
In other words, the same computer-generated genomic constructs assembled through filtering algorithms, reference-sequence fill-ins, and statistical consensus modeling are later treated as the authoritative biological basis for the entire outbreak-response infrastructure itself.
Now, that framework is being used to justify mainstream media messaging and authoritarian quarantine measures imposed by governments on passengers of the Hondius.
Leaving unanswered toxicity concerns and whether vaccine components or material the jab forces the body to produce can spread beyond the recipient.
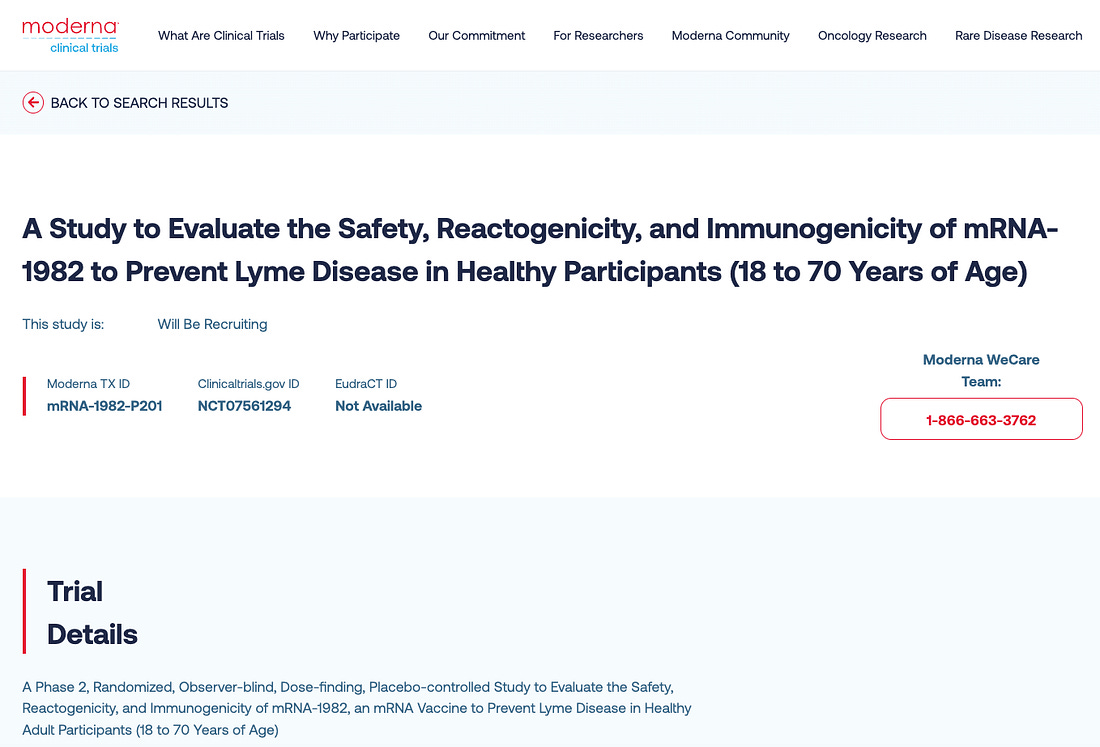
Moderna is preparing to inject approximately 350 people with an experimental mRNA Lyme disease shot as part of a newly listed Phase 2 human clinical trial, according to the company website and ClinicalTrials.gov.
The move comes after Pfizer revived a Lyme vaccine strategy tied to autoimmune arthritis concerns and lawsuits that contributed to the withdrawal of the only previous Lyme shot from the market.
The new Moderna candidate, mRNA-1982, will be evaluated in a randomized, placebo-controlled study involving healthy adults in Canada between the ages of 18 and 70.
The “1982” designation points to the year the Lyme-causing bacterium was formally identified and named, cementing Lyme disease as a defined tick-borne infection.
FDA Commissioner Dr. Marty Makary has asserted that Lyme disease “came from Lab 257 on Plum Island,” directly tying the origin of the illness to a U.S. government lab.
As of the latest update, the mRNA-1982 trial is not yet recruiting, despite an estimated start date of April 27, 2026.
Trial Structure
Participants will receive intramuscular injections of either the mRNA shot or a placebo under a sequential, dose-evaluation design.
The study includes both an initial dosing phase and a booster phase, with monitoring that tracks:
Local and systemic reactions within 7 days
Adverse events through 28 days
Medically attended and serious adverse events for up to 21 months
Target: Lyme-Linked Bacteria
The injection is designed to encode outer surface protein A (OspA), associated with Borrelia, the bacteria linked to Lyme disease.
The program reflects Moderna’s ongoing expansion of mRNA-based products beyond viral applications, like coronavirus, into bacterial targets.
Additional Candidate
Alongside mRNA-1982, the company is developing another Lyme-focused candidate, mRNA-1975, described as a heptavalent formulation intended to target multiple Borrelia serotypes.
Timeline
The Phase 2 study lists an estimated primary and overall completion date of November 2028.
The trial record does not indicate whether Moderna is testing whether vaccine-produced OspA proteins, mRNA, or related biological material can be packaged into extracellular vesicles and released from the body.
That omission matters because a 2021 Journal of Extracellular Vesicles study found that cells expressing a target protein can release extracellular vesicles that “carry” that protein, demonstrating that what is produced inside the body can be exported outside the cell in membrane-bound particles.
A separate 2023 Pharmaceutics review explains that exosomes are natural transport vesicles that carry proteins and nucleic acids throughout the body and are present in bodily fluids including blood, saliva, and other secretions—meaning they are not confined to the original cell or even the original location in the body.
Taken together, the literature establishes that biologically active material produced inside cells can be packaged into vesicles, circulate systemically, and exit the body through bodily fluids.
That raises a direct informed consent issue: whether an mRNA Lyme injection could result in the body producing OspA or other vaccine-related material that is then packaged into exosomes and shed outside the body—creating a potential pathway for transfer to others through close contact or exposure to bodily fluids.
The question is not just what happens inside the person receiving the injection, but whether what their cells are instructed to produce can leave their body and reach someone else.
Moreover, a January 2023 Nature Reviews Drug Discovery paper co-authored by Moderna scientists bluntly admits that avoiding “unacceptable toxicity” in mRNA vaccines remains a major challenge, warning that “lipid nanoparticle structural components, production methods, route of administration and proteins produced from complexed mRNAs all present toxicity concerns” and that the way these vaccines spread through the body can cause harm due to “cell tropism and tissue distribution… and their possible reactogenicity.”
You can contact Moderna here and ask whether the company has addressed these toxicity concerns.
You can also ask whether their Phase 2 Lyme mRNA trial is evaluating if they have confirmed whether or not vaccine-produced OspA proteins or mRNA are packaged into extracellular vesicles, whether those vesicles can enter bodily fluids, and whether any studies have assessed the potential for this material to be shed or transferred to other individuals—and if not, why those risks were not addressed before human injection.
Bottom Line
Moderna is moving ahead with injecting 350 people with an mRNA Lyme shot that turns the body into a producer of bacterial antigen, while failing to immediately address toxicity concerns or whether vaccine components and antigenic material can be packaged, circulated, and shed to others—an unresolved risk at the center of informed consent.
Rep. Schrier’s bill funnels taxpayer cash into Big Pharma, state propaganda, and pediatric surveillance expansion.
Representative Kim Schrier (D-WA) last week introduced H.R. 8425, the “Strengthening the Vaccines for Children Program Act of 2026,” a sweeping federal bill that could funnel billions in taxpayer dollars into an expanded child vaccine control grid.
The legislation does this by deepening federal vaccine infrastructure, increasing payments to vaccine administrators, financially coercing states into running federally approved vaccine propaganda campaigns, and expanding long-term pediatric surveillance systems.
According to campaign finance watchdog OpenSecrets and the Federal Election Commission, Schrier’s donor base includes entities with potential financial or institutional interests in expanded vaccine systems, including:
Pfizer
Abbott Laboratories
Quest Diagnostics
Kaiser Permanente
American Medical Association
Critics view this as a direct conflict of interest, with pharmaceutical and medical industry donors financially backing a lawmaker whose bill could materially benefit the very corporations and healthcare systems funding her political career.
Rep. Schrier introduced H.R. 8425 alongside original cosponsor Rep. John Joyce (R-PA).
H.R. 8425 was immediately referred to the House Committee on Energy and Commerce, where it currently remains in committee after introduction.
Federal Government Uses Medicaid Billions to Pressure States Into Running Vaccine Propaganda
Beginning January 1, 2027, H.R. 8425 offers states a 1% increase in Federal Medical Assistance Percentage (FMAP)—a potentially multi-billion-dollar taxpayer-funded incentive—but only if they comply with federal vaccine messaging mandates.
The bill explicitly states:
“Federal medical assistance percentage determined for each State… under section 1905(b) of the Social Security Act (42 U.S.C. 1396d(b)) shall be increased by 1 percentage point.”
“A State… may not receive the increase… if such State does not ensure culturally competent and effective messages for vaccination outreach to child populations…”
Required messaging includes promotion of:
“advancements in research and vaccine development that have saved millions…”
“the dangers of not being vaccinated…”
“vaccine safety…”
This creates direct federal financial leverage to transform state health departments into taxpayer-funded child vaccine propaganda systems.
Bill Expands Federal Child Vaccine Pipeline Into Millions More Children
The bill broadens federal vaccine system reach by expanding eligibility:
“A child who is enrolled for child health assistance under a State child health plan approved under title XXI.”
This automatically folds CHIP-enrolled children deeper into federally subsidized vaccine programs, expanding the national pediatric vaccine apparatus.
Providers Paid Premium Rates to Push Vaccines—Even When Parents Decline
H.R. 8425 guarantees:
“payment for vaccine administration and counseling services… at a rate not less than 100 percent…”
And providers may bill:
“regardless of whether such vaccine is actually administered”
This means taxpayer dollars can directly reward doctors and healthcare systems for vaccine pressure campaigns even when families refuse injections.
Combination Vaccines Become Bigger Big Pharma Revenue Engines
The bill authorizes:
“a separate charge for the administration of and counseling for each component of such vaccine”
This creates stronger reimbursement incentives for expanded multi-component vaccine schedules, potentially increasing pharmaceutical and provider profits.
Pediatric Surveillance Grid Deepened
The legislation authorizes broader access to:
“data, data sets, monitoring systems, delivery systems, and other protected health information…”
CDC must also publicly track:
“vaccination rates… disaggregated by region, age, sex, race, ethnicity…”
This would significantly expand the federal government’s pediatric surveillance grid by increasing institutional access to protected child health data, strengthening vaccine uptake monitoring systems, and building more powerful demographic tracking infrastructure capable of identifying, targeting, and pressuring under-vaccinated populations with greater precision.
Bottom Line
H.R. 8425 is a major federal expansion of a billion-dollar child vaccine control grid that could:
Funnel taxpayer money into pharmaceutical and provider systems
Financially coerce states into vaccine propaganda compliance
Reward providers for vaccine pressure
Expand federally managed child vaccine pipelines
Build stronger surveillance and demographic compliance tracking systems
For critics focused on medical freedom, parental rights, and government overreach, the bill represents a substantial escalation in the merger of federal power, pharmaceutical profit, and public health surveillance—building the infrastructure today for larger future child vaccine campaigns, broader compliance pressure, and deeper institutional control tomorrow.
USDA, NIAID, and NIH finance genetic experiment generating human avian influenza pathogen from scratch that can infect cows.
A newly published study in npj Veterinary Sciences reveals that federally funded researchers have bioengineered an infectious human H5N1 bird flu pathogen in a Biosafety Level 3 (BSL-3) laboratory and intentionally infected dairy cows.
The new bird flu project received backing from the U.S. Department of Agriculture (USDA), the National Institutes of Health (NIH), and the National Institute of Allergy and Infectious Diseases (NIAID).
According to the study:
“Reverse genetics plasmids for wild-type A/Texas/37/2024 (H5N1)… were obtained from Twist Biosciences.”
“Reverse genetics to generate the infectious clone was performed using the 8-plasmid system… in a Biosafety Level 3 (BSL-3) laboratory.”
Using plasmid-based biotechnology, researchers say they have built a live infectious clone of a human H5N1 bird flu virus inside a federally funded high-containment laboratory.
The study’s listed researchers from the University of Georgia (contact) are: Flavio Cargnin Faccin, L. Claire Gay, Dikshya Regmi, Sasha Compton, Teresa D. Mejías, Juliana Calil Brondani, Lok R. Joshi, Elizabeth W. Howerth, Daniela S. Rajao, Roberto A. Palomares, and Daniel R. Perez.
Scientists Directly Infect Live Dairy Cows
After constructing the pathogen, researchers deliberately exposed cows through both nasal and direct mammary gland infection:
“Cows were inoculated with 1 × 106 TCID50/ml of A/Texas/37/2024 (H5N1), administered as follows: 4 ml instilled into each nostril… and 2 ml in each of two quarters… using a teat cannula.”
Scientists directly introduced the bioengineered virus into cows’ noses and milk-producing udder tissue.
Infection Triggers Severe Biological Damage
Following deliberate infection:
Milk production collapsed by roughly 75%
Milk became yellow and abnormal
Mammary glands developed severe mastitis and tissue destruction
Viral replication surged in milk and udder tissue
Fever spike reached 106°F
Researchers report:
“Milk production rapidly decreased, and milk samples exhibited a colostrum-like appearance.”
“These findings strongly support significant viral replication within infected quarters.”
Human Bird Flu Crosses Directly Into Cattle
Researchers confirm:
“By using a human H5N1 virus, we demonstrated that cows could be infected with a human H5N1 strain.”
Backed by NIH, NIAID, and USDA funding, scientists successfully bioengineered an infectious human H5N1 bird flu virus and demonstrated that it can cross species barriers and infect large mammalian livestock.
Federal Bird Flu Infrastructure Expands Vaccine Development
Researchers explicitly state:
“Our findings confirm that Jersey cows are susceptible to H5N1 infection and establish them as a valuable experimental model for studying disease pathogenesis and vaccine development.”
Federal agencies now expand dairy cattle as a large-animal model for future H5N1 vaccine development and pathogenesis programs.
Federal Funding Streams
Funding includes:
USDA/NIFA
NIH/NIAID
Federal contracts
Government influenza grants
“We thank Julia Grindle and Kilie Wilson for their assistance with milking the cows during the acclimation period. We thank Jazmin Destiny Lynn, Hannah Walker, Karly Pecua, Morgan George, and Robert Gafnea at the Animal Health and Research Center, University of Georgia, specifically for their assistance during animal studies under Animal Biosafety Level 3 containment. Funding for this work includes grants, contracts, and subawards to D.R.P. including National Institute of Food and Agriculture (NIFA), U.S. Department of Agriculture (USDA) Grant award numbers 2020-67015-31539 and 2021-67015-33406, National Institute of Allergy and Infectious Diseases, National Institutes of Health (NIH) Grant award number R21AI146448 and R01AI154894, Contract number 75N93021C00014 and Options 15A, 15B and 17A. Additional funds were provided to D.R.P. by the Georgia Research Alliance and the Caswell S Eidson Chair in Poultry Medicine endowment funds.”
Bottom Line
USDA, NIH, and NIAID actively fund scientists to build a bioengineered human H5N1 bird flu pathogen in a BSL-3 laboratory, prove it can cross species barriers into large mammalian livestock, and deliberately infect dairy cows to expand federal bird flu pathogenesis and vaccine development infrastructure.
The study confirms U.S. government-backed scientists are not only constructing and deploying infectious bird flu pathogens in live animals, but also expanding the biological and operational systems needed for future large-scale influenza experimentation, surveillance, and countermeasure development.
Gov’t finances creation of lethal avian influenza Frankenviruses in Nebraska.
A newly released npj Vaccines study confirms that U.S. government–funded researchers constructed hybrid influenza viruses in the lab and used them to trigger complete mortality in animal experiments, while framing the work under vaccine development.
The experiment, titled “Dual-Route H5N1 Vaccination Induces Systemic and Mucosal Immunity in Murine and Bovine Models,” was conducted by University of Nebraska–Lincoln scientists Joshua Wiggins, Adthakorn Madapong, and Eric A. Weaver.
The creation of deadly chimeric pathogens was financed by the U.S. Department of Agriculture (USDA) and the National Institute of Allergy and Infectious Diseases (NIAID).
The study explicitly states:
“This research was supported by the U.S. Department of Agriculture, National Institute of Food and Agriculture, Agriculture and Food Research Initiative (Grant Nos. 2020 -06448 and 2024 -08723 to E.A.W.), and by the National Institutes of Health –NIAID (Grant No. 1R01AI147109 to E.A.W.).”
The researchers say they constructed the hybrid bird flu pathogens using reverse genetics.
That means the scientists assembled the viruses from scratch by inserting their genetic sequences into plasmids and introducing them into cells, which then are said to produce a fully formed infectious virus.
The paper states:
“A BSL-2 compliant reverse genetic (rg) system was used to produce” H5N1 Influenza A virus strains.”
And details how they were assembled:
“Six (PB1, PB2, PA, NP, M, and NS) IAV gene segments from the PR/8/34 H1N1 laboratory strain were cloned individually into the pHW2000 vector. Separately, the neuraminidase (N) gene and hemagglutinin (H) gene without the highly pathogenic multibasic cleavage site from each strain were synthesized and cloned into the same pHW2000 vector.”
This is a genetic recombination system:
Internal genes from a lab strain (PR/8/34)
Surface genes (H5N1) inserted
Entire virus rebuilt from plasmids
That is a chimeric influenza construct—a hybrid assembled in the lab.
Engineered Pathogens Cause Lethal Disease
Even with deliberate modification of a known virulence element:
“hemagglutinin… without the highly pathogenic multibasic cleavage site”
—the viruses remained lethal.
100% Mortality in Mammals
The outcome in animals exposed to these engineered viruses is stated plainly:
Forces your body to flood bloodstream with antibody proteins that ticks consume during feeding.
Pfizer and Valneva have advanced their experimental Lyme disease vaccine, PF-07307405 (LB6V, formerly VLA15), using the same core biological mechanism that sparked autoimmune arthritis concerns, lawsuits, and the eventual withdrawal of the only previous Lyme vaccine, LYMErix.
The jab works by forcing the body to produce antibodies against a bacterial protein that resembles a protein found in your own joint tissue, meaning those antibodies may also recognize similar structures in your joints and trigger an immune response there.
That means a mechanism previously tied to immune responses against joint tissue—producing Lyme-like symptoms—is now being brought back and positioned for broad public rollout.
Moreover, current data tracks antibody levels in the bloodstream over months, but does not map where those antibodies distribute in human tissues or how repeated boosting affects immune activity over the long term.
The Mechanism Activates Only After a Tick Bites
The vaccine is built to force the body to produce large quantities of anti-OspA IgG antibodies that circulate in the bloodstream.
Those antibodies remain inactive until a tick begins feeding.
At that point, the process engages.
The companies describe it:
“As the tick feeds on the vaccinated person, these antibodies are ingested by the tick as part of its blood meal. Binding of vaccine-induced antibodies to OspA on Borrelia inside the tick inhibits the bacterium’s ability to leave the tick.”
The antibodies are produced in the human body, but their intended function occurs after they are consumed by the tick.
The activity takes place inside the parasite.
Same OspA Design Behind LYMErix
The approach mirrors the OspA-based strategy used in LYMErix, introduced in 1998 and withdrawn in 2002 after widespread controversy.
At the center of that controversy was molecular mimicry.
The OspA protein contains regions that resemble a human protein known as LFA-1 (leukocyte function-associated antigen-1), which is present on immune cells and in joint tissue. A 1998 Science paper (Gross et al.) identified this overlap, showing that immune responses to OspA could also recognize similar structures on human LFA-1.
In patients with treatment-resistant Lyme arthritis, immune responses directed at OspA were observed to cross-react with LFA-1, raising the possibility that antibodies generated against the bacterial protein could also interact with joint tissue.
Autoimmune Arthritis Concerns Drove Lawsuits and Withdrawal
The cross-reactivity concern—antibodies recognizing both bacterial targets and structurally similar human proteins—became a central issue.
Reports of adverse outcomes, combined with media attention and legal action, intensified scrutiny around the vaccine.
A January 2001 New York Times publication explained:
A panel of U.S. experts is set to hear arguments Wednesday about whether a vaccine against Lyme disease may be linked to rare cases of arthritis, a charge the product maker has disputed.
GlaxoSmithKline Plc, the vaccine manufacturer and the world’s largest drug company, said it plans to present information on patients’ experiences since the product debuted under the brand name LYMErix in January 1999.
…
The Food and Drug Administration (FDA) is holding the public meeting to review the product’s safety and update the advisory panel on complaints that LYMErix may be linked to an untreatable type of arthritis.
…
Some scientists theorize that a protein, OspA, in the vaccine may trigger arthritis in patients with a genetic sensitivity to the condition. An estimated 30 percent of people have the gene suspected to put them at risk.
Lawyers have filed suit against GlaxoSmithKline, charging that the company should have warned that some people who receive the vaccine may experience arthritis that resists treatment.
“Because of the hypothesis of molecular mimicry and autoimmune responses to the vaccine, anti-vaccine sentiment and class action lawsuits, a complicated vaccine administration schedule, diminishing physician support for the vaccine, and low public demand for the vaccine; the manufacturer voluntarily terminated vaccine production and marketing of the vaccine in 2002.”
The Vaccine Is Built to Induce the Same Immune Response Behind Lyme Arthritis
Lyme disease is known to produce an immune-driven arthritis in some patients—joint swelling, pain, and inflammation that can persist even after the bacteria are no longer detectable.
At that stage, the symptoms are not being driven by infection.
They are being driven by the immune response itself.
That same category of immune activity sits at the center of the vaccine’s design.
The shot is designed to force the body to generate high levels of anti-OspA antibodies against a bacterial protein that has been shown to share structural similarity with human LFA-1—a protein present in joint tissue.
That overlap places the immune response and the target in the same biological context as Lyme-related joint inflammation.
The result is a direct convergence: the vaccine is engineered to induce the same type of immune response associated with joint inflammation in Lyme disease.
This is the same biological interaction that raised concern during the LYMErix era.
Same Mechanism, Sustained Through Repeated Dosing
The current Pfizer candidate expands the design across six Borrelia serotypes.
Its function depends on maintaining elevated antibody levels in circulation, which decline over time based on earlier clinical data.
Booster doses are used to restore those levels, creating repeated cycles of immune activation centered on the same anti-OspA response.
Each cycle reinforces the same antibody pathway tied to the original controversy.
Autoimmune Monitoring Built Into Trials
A Phase 2 booster study published in The Lancet Infectious Diseases monitored participants for autoimmune and neuroinflammatory conditions—the same category of concern associated with the earlier vaccine.
Reported events were assessed by investigators—who worked for Pfizer—as unrelated to the vaccine.
The underlying interaction of antibodies targeting a bacterial protein with structural similarity to human tissue remains unchanged.
Critical Data Gap the Companies Aren’t Addressing
Current trials primarily track antibody levels in the bloodstream over limited time windows.
They have not mapped in detail where these anti-OspA antibodies distribute in human tissues, especially in joints and other sites where LFA-1 is expressed.
There is also no multi-year human data showing how repeated annual boosting affects immune activity over extended periods.
In practical terms, antibody levels in the blood are measured, but tissue-level behavior and long-term immune effects under repeated stimulation are not directly tracked.
This is the same blind spot that existed during the LYMErix era, before concerns around immune-mediated joint effects escalated into broader scrutiny.
Now Pfizer and Valneva are advancing the same mechanism, expanded across more strains and structured around repeated dosing, while those same unanswered questions remain.
Pfizer Felony
Pfizer is a massively criminal enterprise, repeatedly convicted and fined billions for systemic illegal activities, including off-label marketing, safety violations, bribery, price-fixing, and healthcare fraud.
With over $10 billion in penalties since 2002, Pfizer has a proven pattern of habitual corporate crime driven by profit at the expense of public health and legality.
Pfizer has pleaded guilty to felony criminal charges, including in 2009 when its subsidiary Pharmacia & Upjohn pleaded guilty to a felony count of misbranding pharmaceuticals.
The company agreed to pay a record $2.3 billion criminal and civil settlement for illegal marketing and healthcare fraud, confirming its status as a convicted corporate felon.
That same company is now rolling out a new Lyme vaccine built on the same mechanism that previously ignited safety concerns, lawsuits, and a full market collapse.
Bottom Line
Pfizer’s Lyme vaccine revives the same OspA antibody mechanism that triggered autoimmune arthritis concerns, lawsuits, and market collapse.
It is built around inducing the same category of immune response associated with Lyme-related joint inflammation.
That response is reinforced through repeated dosing.
And the mechanism itself is designed to activate only after antibodies produced in the bloodstream are consumed by a feeding tick.
Follows California, Illinois, Colorado, and New York City’s entry into same transnational WHO outbreak coordination system.
Governor Bob Ferguson announced this month that Washington State is now part of the World Health Organization Global Outbreak and Response Network (GOARN), an international syndicate of “public health agencies, national governments, academic centers, laboratories, and response organizations focused on rapidly detecting and responding to public health emergencies,” according to a press release from the Washington State Nurses Association (WSNA).
Washington joins California, Illinois, Colorado, and New York City by entering GOARN.
According to WSNA, Washington’s public health leaders will fall in line with the WHO’s:
global outbreak early-warning alerts, meaning real-time surveillance tied into an international detection system
technical collaboration and support during major public health events, meaning coordinated response across jurisdictions
international training, exercises, and best-practice exchanges, meaning standardized response protocols
and coordinated outbreak response support, meaning integrated deployment during declared emergencies.
Congress has already confirmed that the WHO’s response to the COVID-19 pandemic “was an abject failure” and that the WHO’s “newest effort to solve the problems exacerbated by the COVID-19 pandemic — via a “Pandemic Treaty” — may harm the United States.”
This means Washington’s decision comes despite federal findings that the WHO mismanaged the last pandemic and is advancing new agreements that could expand its influence over future responses.
You can contact Gov. Ferguson’s office here to voice your opposition to Washington’s integration into a WHO-linked outbreak surveillance and response system and demand accountability for aligning state public health infrastructure with failed global coordination mechanisms.
In the governor’s press release, Washington State Secretary of Health Dennis Worsham cited avian influenza (“bird flu”) in justifying the move:
“Disease outbreaks don’t stop at state or national borders, and our ability to protect people in Washington shouldn’t either,” Washington State Secretary of Health Dennis Worsham said. “Joining GOARN ensures we maintain access to critical global outbreak intelligence and stay connected to leading public health experts, even as federal relationships change. We’re not waiting for the next threat — we’re preparing for it. From COVID-19 to rising measles cases and avian influenza, we’ve seen how quickly diseases can spread. Through GOARN, we can detect risks earlier, respond faster and better protect people in our communities — while also contributing Washington’s expertise to global response efforts.”
The development comes as bird flu is being framed internationally as an imminent threat while laboratory manipulation of the virus continues, vaccines are developed in parallel, and global, federal, and state systems are aligned to respond.
This is the same sequence of surveillance, lab work, and countermeasure rollout that preceded the COVID-19 pandemic.
HHS-backed research produced chimeric influenza viruses carrying SARS-CoV-2’s ACE2-binding interface—introducing a higher-affinity human receptor-binding mechanism into an influenza pathogen.
HHS-funded researchers are claiming to have engineered influenza-based chimeric “Frankenstein” viruses that combine influenza’s hemagglutinin (HA) with the SARS-CoV-2 receptor-binding domain (RBD)—a high-affinity human ACE2-binding interface.
Introducing a fundamentally different and stronger human cell–binding mechanism into an influenza viral system is a modification that fits longstanding U.S. gain-of-function definitions involving altered receptor usage and host range.
A December 2025 bioRxiv preprint confirms the work, supported in part by the National Institutes of Health (NIH)—an agency within the U.S. Department of Health and Human Services (HHS)—was funded under grant P01-AI165075:
“This work was funded by… National Institutes of Health… P01-AI165075”
and involved replacing influenza’s native HA gene with the SARS-CoV-2 RBD while producing virus particles coated with HA in the laboratory, resulting in viral constructs that physically contain both influenza’s entry protein and the SARS-CoV-2 optimized human cell–binding interface.
The study was conducted by Jonathan Munro, Diana Melnyk, Madeeha Afzal, Lisa Schimanski, Alexander A. Cohen, Jennifer R. Keeffe, Pamela J. Bjorkman, William S. James, Alain R. Townsend, and Tiong Kit Tan, with affiliations including the University of Oxford’s Weatherall Institute of Molecular Medicine and Sir William Dunn School of Pathology (here), the Chinese Academy of Medical Sciences–Oxford Institute (here), and the California Institute of Technology (here).
The head of HHS is Secretary Robert F. Kennedy Jr., while NIH is led by Director Jay Bhattacharya and NIAID is headed by Director Jeffery Taubenberger.
Meanwhile, President Donald Trump recently signed legislation into law allocating at least $5.5 billion in taxpayer funding for a future influenza pandemic.
At the same time, the Trump administration has advanced a $500 million “next-generation, gold-standard” combination influenza-COVID vaccine platform—positioning federal agencies to simultaneously fund the development of pandemic-capable influenza-COVID pathogens while building the mass vaccination infrastructure designed to respond to the very outbreak those systems could enable.
Engineered Virus Introduces High-Affinity Human Receptor Binding Into Influenza Backbone
The study explicitly confirms that influenza’s native receptor-binding gene was removed and replaced:
“the native haemagglutinin (HA) sequence is replaced with the coding sequence of… the receptor-binding domain (RBD) of the… SARS-CoV-2”
Influenza viruses naturally infect human cells using hemagglutinin, which binds sialic acid receptors with relatively low individual affinity and relies on multivalent interactions across many HA proteins.
By contrast, the SARS-CoV-2 receptor-binding domain binds directly to the human ACE2 receptor through a high-affinity protein–protein interaction, enabling efficient attachment to human airway cells.
By inserting the SARS-CoV-2 RBD into an influenza backbone, the researchers introduced a human ACE2-binding interface into a virus that does not naturally use that receptor system.
Chimeric Particles Combine Influenza HA and SARS-CoV-2 RBD
The study explicitly states that the influenza virus was genetically modified by replacing its HA coding sequence with the SARS-CoV-2 receptor-binding domain:
“we replaced the native HA coding sequence”
and:
“In this study, we describe the generation of a non-replicating pseudotyped influenza A virus (S-FLU), where the native haemagglutinin (HA) sequence is replaced with the coding sequence of either a membrane-anchored form (TM) or secretory form (Sec) of the receptor-binding domain (RBD) of the ancestral SARS-CoV-2 Wuhan (S-RBD Wuhan).”
At the same time, the study makes clear that HA function is not eliminated at the particle level, but instead supplied externally:
“Inactivation of the native haemagglutinin (HA) signal sequence means that S-FLU can only replicate in cell lines transfected to express HA that provide the surface protein for budding viral particles.”
The authors also confirm that the resulting engineered virus retains the ability to enter cells:
“Notably, S-FLU exhibits the capacity to infect host cells but is replication-incompetent.”
Study Confirms Infection & Expression of SARS-CoV-2 Binding Domain
The researchers confirmed that the engineered virus successfully infected cells and expressed the inserted RBD:
“both S-RBD-TM and S-RBD-Sec led to expression of RBD in the infected cells”
This demonstrates that the chimeric virus delivers and expresses the SARS-CoV-2 receptor-binding domain inside host cells following infection.
Bottom Line
HHS-funded researchers say they have engineered influenza-based viruses that combine influenza’s hemagglutinin (HA) with the SARS-CoV-2 receptor-binding domain (RBD).
They replaced the HA gene with the RBD.
But they still produced virus particles coated with HA.
The result is a chimera that physically carries both influenza’s entry machinery and a high-affinity human ACE2-binding interface.
The study confirms these viruses infect cells and express the RBD.
That is a direct change in receptor usage, consistent with longstanding U.S. gain-of-function definitions.
The work was funded under NIH grant P01-AI165075.
At the same time, the federal government is allocating at least $5.5 billion for an influenza pandemic and advancing a $500 million influenza-COVID vaccine platform—building both the engineered viral systems and the mass-response infrastructure in parallel.
After state’s vaccine passport era, Hawaii lawmakers want to give Department of Health final authority over medical decisions while blocking lawsuits and discipline against those who enforce them.
Hawaii lawmakers are advancing a bill that gives the state’s Department of Health decisive control over which vaccines and preventive services count as medically valid—and then protects anyone who carries them out from nearly all legal consequences.
House Bill 1898 (S.D. 1) creates immunity from civil lawsuits, criminal liability, and professional discipline for providers who follow DOH recommendations on “clinical preventive services.”
If harm occurs later, the main legal question becomes whether the provider obeyed state guidance.
During the next outbreak or pandemic, when the DOH again requires vaccination to work, attend school, travel, or participate in society, anyone injured by the shot could have no one to hold accountable—because the bill grants legal immunity to every doctor, pharmacist, and facility that simply followed state orders.
Watchdog groups actively monitoring the CDC’s Vaccine Adverse Event Reporting System (VAERS) data confirm 2.7 million adverse events have been linked to vaccines since 1990 (~204 adverse events per day)—though a Harvard Pilgrim Health Care report found that fewer than 1% of adverse events are ever reported, suggesting the true number could be in the hundreds of millions (~20,360 adverse events per day).
The bill directly undermines several longstanding health-freedom principles:
Bodily Autonomy and Informed Consent: Full insurance coverage and legal protection are available only for DOH-approved interventions. Families who prefer a different schedule or approach must pay out of pocket for alternatives that carry no such protections.
Medical Accountability: The bill states that “[n]o person shall be subject to civil or criminal liability or professional disciplinary action” for providing services in accordance with DOH recommendations. Professional organizations, hospitals, and licensing boards are barred from disciplining, suspending, or penalizing providers who follow the state line.
Independent Medical Judgment: Doctors who disagree with the DOH’s final decision on immunizations risk professional repercussions, while those who comply are shielded.
Parental Rights in Child Health Decisions: The bill rewrites child health supervision rules so that “prevailing medical standards” now mean whatever the DOH says. Insurance must cover the DOH-chosen immunizations at no cost to the family, leaving parents who want a different schedule to pay full price.
Separation of Medicine and State: Standing orders, mandatory insurance coverage with no cost-sharing, pharmacy administration, and legal immunity combine to create a single state-directed pipeline for preventive care.
Department of Health Given Final Authority
The bill makes the Hawaii Department of Health the tie-breaker when national medical groups disagree.
It states that if recommendations from the Advisory Committee on Immunization Practices and the American Academy of Pediatrics differ, “the department of health shall determine which recommendations shall apply.”
It also gives the DOH new power to issue standing orders for medications and immunizations, allowing them to be given without an individual doctor’s prescription.
Legal Protection Tied to Following State Guidance
The immunity language is clear:
“No professional organization or association, health care provider, or health care facility shall subject any person to discipline, suspension, loss of license, loss of privileges, loss of membership, or other penalty for providing clinical preventive services in accordance with recommendations made pursuant to section 321-31.”
Insurance Must Cover DOH-Approved Services at No Cost
For policies issued after January 1, 2027, insurers must provide coverage “without any deductible, copayment, coinsurance, or other cost-sharing requirements” for anything the DOH recommends.
Every Hawaii policyholder will likely pay higher premiums to subsidize the DOH’s choices—while families who want a different schedule get zero coverage and pay 100% out of pocket.
Pharmacies Can Administer Vaccines Under DOH Rules
HB1898 expands who can give vaccines by allowing pharmacists, pharmacy interns, and registered pharmacy technicians to administer them when ordered in line with DOH recommendations or standing orders.
What This Means in a Future Outbreak
If the DOH issues new recommendations during the next public-health emergency, those shots or treatments can be rolled out quickly through pharmacies, must be covered by insurance, and anyone administering them is protected from lawsuits or discipline as long as they followed DOH guidance.
Negligence Exception Exists, But Standard Is Compliance
The bill still allows claims for injury “arising from negligence.”
In practice, however, the legal test will center on whether the provider followed the Department of Health’s recommendations.
Bottom Line
HB 1898 gives the Department of Health the power to decide which preventive medical interventions are covered and protected by law.
It forces insurers to pay for the state’s choices with no patient cost-sharing and removes meaningful accountability for providers who follow those choices.
Hawaii families who want options outside the official schedule will face higher costs and fewer willing providers.
When the state controls the definition of medical truth and shields its enforcers from consequences, bodily autonomy and informed consent become conditional on government approval rather than individual rights.

























Recent Comments