After WHO—also funded by Gates—declares Ebola a “public health emergency of international concern” and calls for vaccine development, raising conflict-of-interest concerns.
The Bill Gates-funded Coalition for Epidemic Preparedness Innovations (CEPI) will “urgently accelerate development of three investigational vaccines targeting the Bundibugyo Ebola virus that has caused a rapidly spreading epidemic in the Democratic Republic of the Congo (DRC) and neighboring Uganda,” according to a Sunday press release from the organization.
The move comes as the World Health Organization (WHO), also funded by Bill Gates, just weeks ago declared Ebola currently represents a “public health emergency of international concern (PHEIC)” and that there is a need to “[i]mplement clinical trials to advance the development and use of candidate therapeutics and vaccine, supported by partners.”
CEPI now believes there is a “critical need to produce tools to help curtail the outbreak, complementing ongoing public health interventions by affected countries.”
The arrangement raises obvious conflict-of-interest concerns, as Bill Gates-funded transnational health organizations are simultaneously framing the outbreak response, declaring international emergency status, and accelerating the development and deployment of the very vaccine platforms their aligned networks support and finance.
The three vaccine candidates include those developed by the International AIDS Vaccine Initiative (IAVI), Moderna, and the University of Oxford.
CEPI has committed $50 million to Moderna (mRNA platform), $8.6 million to the University of Oxford (adenoviral vector platform), and $3.2 million to IAVI (rVSV vaccine platform).
The press release confirms Moderna’s Ebola formulation will be based on mRNA, like its COVID-19 jab:
“CEPI has committed up to US$50 million for preclinical testing and Phase 1 clinical trials. CEPI will support simultaneous manufacturing of doses to enable large-scale Phase 2/3 trials to begin immediately if Phase 1 data supports progression. This candidate uses the same fast, flexible, scalable mRNA technology validated during COVID-19 and builds upon Moderna’s existing R&D on related Ebola viruses. The collaboration leverages CEPI’s existing strategic partnership with Moderna.”
The same Gates-funded global health network shaping international Ebola messaging, emergency declarations, and government outbreak response is also funding and accelerating the vaccines being presented as the solution to the crisis.
The arrangement raises obvious conflict-of-interest concerns, as the organizations influencing public fear, policy, and emergency infrastructure are financially and operationally tied to the very pharmaceutical platforms being advanced in response.
HHS-backed research produced chimeric influenza viruses carrying SARS-CoV-2’s ACE2-binding interface—introducing a higher-affinity human receptor-binding mechanism into an influenza pathogen.
HHS-funded researchers are claiming to have engineered influenza-based chimeric “Frankenstein” viruses that combine influenza’s hemagglutinin (HA) with the SARS-CoV-2 receptor-binding domain (RBD)—a high-affinity human ACE2-binding interface.
Introducing a fundamentally different and stronger human cell–binding mechanism into an influenza viral system is a modification that fits longstanding U.S. gain-of-function definitions involving altered receptor usage and host range.
A December 2025 bioRxiv preprint confirms the work, supported in part by the National Institutes of Health (NIH)—an agency within the U.S. Department of Health and Human Services (HHS)—was funded under grant P01-AI165075:
“This work was funded by… National Institutes of Health… P01-AI165075”
and involved replacing influenza’s native HA gene with the SARS-CoV-2 RBD while producing virus particles coated with HA in the laboratory, resulting in viral constructs that physically contain both influenza’s entry protein and the SARS-CoV-2 optimized human cell–binding interface.
The study was conducted by Jonathan Munro, Diana Melnyk, Madeeha Afzal, Lisa Schimanski, Alexander A. Cohen, Jennifer R. Keeffe, Pamela J. Bjorkman, William S. James, Alain R. Townsend, and Tiong Kit Tan, with affiliations including the University of Oxford’s Weatherall Institute of Molecular Medicine and Sir William Dunn School of Pathology (here), the Chinese Academy of Medical Sciences–Oxford Institute (here), and the California Institute of Technology (here).
The head of HHS is Secretary Robert F. Kennedy Jr., while NIH is led by Director Jay Bhattacharya and NIAID is headed by Director Jeffery Taubenberger.
Meanwhile, President Donald Trump recently signed legislation into law allocating at least $5.5 billion in taxpayer funding for a future influenza pandemic.
At the same time, the Trump administration has advanced a $500 million “next-generation, gold-standard” combination influenza-COVID vaccine platform—positioning federal agencies to simultaneously fund the development of pandemic-capable influenza-COVID pathogens while building the mass vaccination infrastructure designed to respond to the very outbreak those systems could enable.
Engineered Virus Introduces High-Affinity Human Receptor Binding Into Influenza Backbone
The study explicitly confirms that influenza’s native receptor-binding gene was removed and replaced:
“the native haemagglutinin (HA) sequence is replaced with the coding sequence of… the receptor-binding domain (RBD) of the… SARS-CoV-2”
Influenza viruses naturally infect human cells using hemagglutinin, which binds sialic acid receptors with relatively low individual affinity and relies on multivalent interactions across many HA proteins.
By contrast, the SARS-CoV-2 receptor-binding domain binds directly to the human ACE2 receptor through a high-affinity protein–protein interaction, enabling efficient attachment to human airway cells.
By inserting the SARS-CoV-2 RBD into an influenza backbone, the researchers introduced a human ACE2-binding interface into a virus that does not naturally use that receptor system.
Chimeric Particles Combine Influenza HA and SARS-CoV-2 RBD
The study explicitly states that the influenza virus was genetically modified by replacing its HA coding sequence with the SARS-CoV-2 receptor-binding domain:
“we replaced the native HA coding sequence”
and:
“In this study, we describe the generation of a non-replicating pseudotyped influenza A virus (S-FLU), where the native haemagglutinin (HA) sequence is replaced with the coding sequence of either a membrane-anchored form (TM) or secretory form (Sec) of the receptor-binding domain (RBD) of the ancestral SARS-CoV-2 Wuhan (S-RBD Wuhan).”
At the same time, the study makes clear that HA function is not eliminated at the particle level, but instead supplied externally:
“Inactivation of the native haemagglutinin (HA) signal sequence means that S-FLU can only replicate in cell lines transfected to express HA that provide the surface protein for budding viral particles.”
The authors also confirm that the resulting engineered virus retains the ability to enter cells:
“Notably, S-FLU exhibits the capacity to infect host cells but is replication-incompetent.”
Study Confirms Infection & Expression of SARS-CoV-2 Binding Domain
The researchers confirmed that the engineered virus successfully infected cells and expressed the inserted RBD:
“both S-RBD-TM and S-RBD-Sec led to expression of RBD in the infected cells”
This demonstrates that the chimeric virus delivers and expresses the SARS-CoV-2 receptor-binding domain inside host cells following infection.
Bottom Line
HHS-funded researchers say they have engineered influenza-based viruses that combine influenza’s hemagglutinin (HA) with the SARS-CoV-2 receptor-binding domain (RBD).
They replaced the HA gene with the RBD.
But they still produced virus particles coated with HA.
The result is a chimera that physically carries both influenza’s entry machinery and a high-affinity human ACE2-binding interface.
The study confirms these viruses infect cells and express the RBD.
That is a direct change in receptor usage, consistent with longstanding U.S. gain-of-function definitions.
The work was funded under NIH grant P01-AI165075.
At the same time, the federal government is allocating at least $5.5 billion for an influenza pandemic and advancing a $500 million influenza-COVID vaccine platform—building both the engineered viral systems and the mass-response infrastructure in parallel.
After state’s vaccine passport era, Hawaii lawmakers want to give Department of Health final authority over medical decisions while blocking lawsuits and discipline against those who enforce them.
Hawaii lawmakers are advancing a bill that gives the state’s Department of Health decisive control over which vaccines and preventive services count as medically valid—and then protects anyone who carries them out from nearly all legal consequences.
House Bill 1898 (S.D. 1) creates immunity from civil lawsuits, criminal liability, and professional discipline for providers who follow DOH recommendations on “clinical preventive services.”
If harm occurs later, the main legal question becomes whether the provider obeyed state guidance.
During the next outbreak or pandemic, when the DOH again requires vaccination to work, attend school, travel, or participate in society, anyone injured by the shot could have no one to hold accountable—because the bill grants legal immunity to every doctor, pharmacist, and facility that simply followed state orders.
Watchdog groups actively monitoring the CDC’s Vaccine Adverse Event Reporting System (VAERS) data confirm 2.7 million adverse events have been linked to vaccines since 1990 (~204 adverse events per day)—though a Harvard Pilgrim Health Care report found that fewer than 1% of adverse events are ever reported, suggesting the true number could be in the hundreds of millions (~20,360 adverse events per day).
The bill directly undermines several longstanding health-freedom principles:
Bodily Autonomy and Informed Consent: Full insurance coverage and legal protection are available only for DOH-approved interventions. Families who prefer a different schedule or approach must pay out of pocket for alternatives that carry no such protections.
Medical Accountability: The bill states that “[n]o person shall be subject to civil or criminal liability or professional disciplinary action” for providing services in accordance with DOH recommendations. Professional organizations, hospitals, and licensing boards are barred from disciplining, suspending, or penalizing providers who follow the state line.
Independent Medical Judgment: Doctors who disagree with the DOH’s final decision on immunizations risk professional repercussions, while those who comply are shielded.
Parental Rights in Child Health Decisions: The bill rewrites child health supervision rules so that “prevailing medical standards” now mean whatever the DOH says. Insurance must cover the DOH-chosen immunizations at no cost to the family, leaving parents who want a different schedule to pay full price.
Separation of Medicine and State: Standing orders, mandatory insurance coverage with no cost-sharing, pharmacy administration, and legal immunity combine to create a single state-directed pipeline for preventive care.
Department of Health Given Final Authority
The bill makes the Hawaii Department of Health the tie-breaker when national medical groups disagree.
It states that if recommendations from the Advisory Committee on Immunization Practices and the American Academy of Pediatrics differ, “the department of health shall determine which recommendations shall apply.”
It also gives the DOH new power to issue standing orders for medications and immunizations, allowing them to be given without an individual doctor’s prescription.
Legal Protection Tied to Following State Guidance
The immunity language is clear:
“No professional organization or association, health care provider, or health care facility shall subject any person to discipline, suspension, loss of license, loss of privileges, loss of membership, or other penalty for providing clinical preventive services in accordance with recommendations made pursuant to section 321-31.”
Insurance Must Cover DOH-Approved Services at No Cost
For policies issued after January 1, 2027, insurers must provide coverage “without any deductible, copayment, coinsurance, or other cost-sharing requirements” for anything the DOH recommends.
Every Hawaii policyholder will likely pay higher premiums to subsidize the DOH’s choices—while families who want a different schedule get zero coverage and pay 100% out of pocket.
Pharmacies Can Administer Vaccines Under DOH Rules
HB1898 expands who can give vaccines by allowing pharmacists, pharmacy interns, and registered pharmacy technicians to administer them when ordered in line with DOH recommendations or standing orders.
What This Means in a Future Outbreak
If the DOH issues new recommendations during the next public-health emergency, those shots or treatments can be rolled out quickly through pharmacies, must be covered by insurance, and anyone administering them is protected from lawsuits or discipline as long as they followed DOH guidance.
Negligence Exception Exists, But Standard Is Compliance
The bill still allows claims for injury “arising from negligence.”
In practice, however, the legal test will center on whether the provider followed the Department of Health’s recommendations.
Bottom Line
HB 1898 gives the Department of Health the power to decide which preventive medical interventions are covered and protected by law.
It forces insurers to pay for the state’s choices with no patient cost-sharing and removes meaningful accountability for providers who follow those choices.
Hawaii families who want options outside the official schedule will face higher costs and fewer willing providers.
When the state controls the definition of medical truth and shields its enforcers from consequences, bodily autonomy and informed consent become conditional on government approval rather than individual rights.
L.D. 2071 requires pharmacists to report each vaccine within 72 hours to a centralized state system, enabling real-time monitoring of vaccination across the population.
Maine lawmakers have passed legislation that fundamentally restructures how influenza vaccines can be deployed across the state—establishing a system capable of rapid, large-scale distribution to the general population without relying on physicians.
The final version of L.D. 2071 gives pharmacists full independent authority to prescribe, dispense, and administer influenza vaccines to individuals as young as 3 years and 6 months old—without a prescription or prior medical approval.
This structure removes physician oversight, concentrates vaccination authority in retail pharmacies, and pairs rapid, population-wide access with centralized state reporting—raising concerns about informed consent, medical autonomy, and the state’s ability to execute a fast, large-scale influenza vaccination campaign if another public health emergency is declared.
As of April 7, 2026, the bill has passed both chambers in identical final form and has been ordered sent to the Governor’s desk for signature.
The bill will take effect 90 days after the Legislature adjourns, which is scheduled for April 15, 2026—meaning the new pharmacist authority would become law on July 14, 2026.
The legislation’s advancement comes amid state, federal, and international influenza outbreak orchestration.
Pharmacists Become Frontline Vaccination Authority
Under the amended statute:
“A pharmacist… may prescribe, dispense or administer… all forms of influenza vaccines… to a person 3 years 6 months of age or older without a prescription.”
This language removes the traditional requirement that a physician authorize vaccination—transferring full control over influenza vaccine delivery directly to retail pharmacies.
Pharmacists are no longer limited to administering a doctor’s order.
They can now initiate vaccination themselves.
That shift transforms pharmacies from passive distribution points into independent vaccination hubs capable of operating at scale.
Statewide Retail Network Activated for Mass Deployment
By design, the system leverages the existing pharmacy network as the backbone of vaccine delivery.
Instead of relying on:
clinics
hospital systems
scheduled appointments
The law enables:
walk-in access
immediate administration
decentralized distribution
Pharmacies—already embedded in nearly every community—function as a ready-made infrastructure for rapid statewide rollout.
Influenza Singled Out for Broadest Authority
The legislation treats influenza differently from all other vaccines.
Influenza vaccines:
pharmacist can prescribe, dispense, and administer
applies down to age 3 years 6 months
Other vaccines:
independent pharmacist authority limited to adults 18+
minors require a doctor’s prescription
This makes influenza the only vaccine category granted full pharmacist-controlled access across both adults and young children.
Real-Time State Tracking Built In
The bill also requires that every administered vaccine be reported:
Pharmacists must report vaccine administration to the state immunization information system within 72 hours.
This creates a centralized system capable of:
tracking vaccination rates
monitoring geographic uptake
identifying gaps in coverage
The result is near real-time visibility into how widely vaccines are being administered across the population.
Insurance Language Opens the Door—Without Mandating Coverage
While earlier versions of the bill proposed mandatory no-cost vaccine coverage, the final version stops short of requiring it.
Instead, the amended law clarifies that insurers are authorized to cover vaccines without cost-sharing if they choose, rather than mandating it.
Even without a mandate, the structure aligns financial incentives with expanded access.
What the Structure Reveals
The bill establishes:
Immediate, walk-in vaccination access
No physician gatekeeping
A statewide pharmacy-based delivery network
Rapid reporting into a centralized tracking system
Inclusion of young children in the rollout model
This represents a complete redesign of how influenza vaccines can be deployed at scale.
Bottom Line
Maine legislators have constructed a system that allows influenza vaccines to be distributed quickly, broadly, and with minimal friction across the entire population.
If activated, the infrastructure enables any individual to walk into a pharmacy, receive an influenza vaccine on the spot, and have that dose logged into a statewide tracking system within days—without ever interacting with a physician.
H.R. 7973, with 203 cosponsors, would create a closed-loop federal system to identify pregnant women by race and demographics, boost their vaccination rates, and track them in real time.
A federal bill introduced in Congress would create a system where pregnant women are not only targeted for increased vaccination but also tracked through a federally coordinated surveillance network that activates during pandemics.
H.R. 7973—the “Momnibus Act”—authorizes a staggering $2.46 billion overall, with $715 million of that specifically allocated to build this structure: combining mass vaccination initiatives with a real-time data tracking system designed to monitor health status, outcomes, and demographic characteristics during declared public health emergencies.
The bill constructs a pipeline to identify the population, increase medical intervention, and track the results—continuously, at scale, and under federal coordination.
From a health freedom standpoint, this represents a shift away from individual consent-driven care and toward a system where specific populations are identified, targeted, and monitored during crises.
Introduced by Rep. Lauren Underwood—Backed by Industries Positioned to Benefit
It remains at the earliest stage of the legislative process, with no hearings or votes.
Campaign finance data shows support from healthcare systems, insurance networks, and pharmaceutical-aligned interests—industries that would directly benefit from:
expanded vaccination programs
increased federal funding streams
long-term surveillance infrastructure
The same entities positioned to carry out the bill’s mandates are among those funding its sponsor.
You can contact Rep. Underwood here and the rest of the bill’s 203 cosponsors here to voice your opposition to the expansion of federally directed vaccination targeting, real-time health surveillance during public health emergencies, demographic-based population profiling, centralized control over medical data and response, and the erosion of informed consent and individual medical autonomy.
Federal Government Moves to Identify & Increase Vaccination in Targeted Populations
The bill directs federal agencies to “increase vaccination rates of pregnant and postpartum individuals… and their children.”
Funding is explicitly tied to expanding these efforts, with hundreds of millions authorized specifically for awareness and equity campaigns that prioritize populations with “low rates of vaccination” and “racial and ethnic minority groups.”
The federal government is authorized to identify which groups are not complying with recommended vaccination schedules and focus massive resources on increasing uptake in those populations.
That is a shift from informed consent at the individual level to behavioral targeting at the population level.
$715 Million Surveillance & Vaccine Apparatus Designed for Pandemic Activation
Of the bill’s $2.46 billion total authorizations, $715 million goes directly to the combined maternal vaccine push and surveillance system:
$190 million for CDC maternal surveillance system, expanded mortality/morbidity tracking, national pregnancy risk monitoring, and NIH emergency research.
The remaining hundreds of millions are dedicated to the maternal vaccination awareness and equity campaign (including the updated $73.4 million per year authorization for 2027–2032).
The system will be used for “data collection, surveillance, and research… as a result of public health emergencies and infectious diseases.”
Real-Time Monitoring of Medical Status During Emergencies
The system tracks “diagnostic testing, confirmed cases, hospitalizations, deaths…” with updates required “at least on a monthly basis.”
This creates continuous, rolling surveillance of a defined population during a declared emergency.
In practical terms, once an emergency is declared, the federal system gains ongoing visibility into who is infected, who is hospitalized, and how individuals are progressing.
That is real-time population monitoring tied directly to health status.
Nationwide Data Integration—From Lab to Federal Database
The bill requires “capacity building… to collect and transmit… demographic data” and mandates that laboratories receive “race, ethnicity, pregnancy status… and other demographic data.”
This creates a standardized data pipeline: data originates at testing sites and hospitals, moves through state systems, and is centralized at the federal level.
Mandatory Demographic Profiling of Health Data
All collected data must be categorized by “race, ethnicity, gender, primary language, geography, socioeconomic status.”
Rather than just tracking disease, the bill would allow tracking of mothers who have the disease, where they are, and what demographic group they belong to.
That enables targeted interventions and creates a framework for population-level categorization tied to medical status.
Centralized Data Collection Before Public Release
The bill requires public reporting on the CDC website while stating “all data collected is deidentified.”
The key distinction is timing.
Data is collected in detailed individual form first, then anonymized before public release.
Federal Authority Expands Immediately After Emergency Declaration
Within 30 days of a public health emergency, “the Secretary shall issue guidance.”
This allows federal officials to control how states collect data, categorize individuals, and manage reporting systems.
A Closed-Loop System: Identify, Intervene, Track
The structure of the bill connects three functions into one system:
Identify populations through demographic data
Increase vaccination rates within those populations
Track outcomes during infectious disease events
This creates a feedback loop where data identifies targets, programs drive intervention, surveillance measures compliance and outcomes.
All operating under federal coordination during a public health emergency.
Bottom Line
H.R. 7973 establishes a federally coordinated $715 million system (within a $2.46 billion bill) that:
identifies specific populations of pregnant and postpartum women for increased vaccination
tracks their medical status in real time during pandemics
categorizes individuals by demographic characteristics
integrates data across labs, hospitals, and government systems
centralizes authority during declared emergencies
The bill lays the groundwork for a model where medical decisions are no longer purely individual—but increasingly shaped by population-level targeting, centralized guidance, and continuous monitoring during crises.
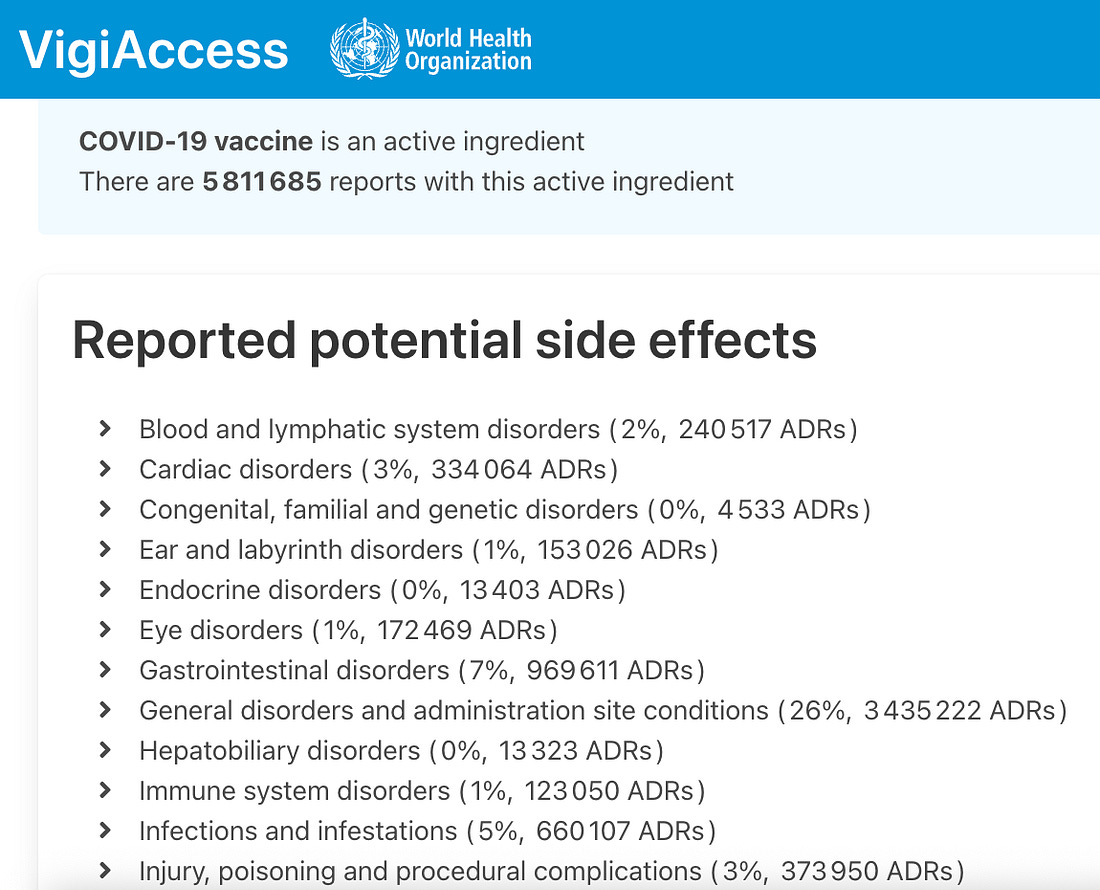
World Health Organization data show system-wide adverse event reports spanning neurological, cardiac, immune, gastrointestinal, and reproductive categories.
The World Health Organization’s VigiAccess pharmacovigilance database currently lists 5,811,685 individual adverse drug reaction (ADR) reports associated with COVID-19 vaccines as an active ingredient.
A Harvard Pilgrim Healthcare/HHS study confirms fewer than 1% of vaccine adverse events are reported, meaning the number could be closer to half a billion.
These reports are submitted by national drug regulators worldwide and categorized by affected body system.
Below is the full numerical breakdown exactly as listed in the database.
Reported Potential Side Effects by System Category
General disorders and administration site conditions 3,435,222 reports (26%)
“A PCR-positive test alone can by no means confirm infection,” study authors confirm—yet the test is currently being used to justify government response to bird flu.
Only a small fraction of people who tested positive for COVID-19 by PCR in Germany met researchers’ criteria for infection, according to an October peer-reviewed study published in Frontiers in Epidemiology.
The findings come as PCR tests are being used to justify government response to avian influenza “bird flu,” including animal culling, countermeasures (vaccine) development, and gain-of-function experiments.
After analyzing nationwide laboratory data from March 2020 through mid-2021, the authors of the new study concluded that only 14% of PCR-positive individuals showed evidence of true infection, which they measured by later antibody development.
The remaining majority did not.
“Only approximately 14% of those who tested PCR-positive were actually infected.”
That means 86% of PCR-positive tests did not meet the authors’ definition of infection, calling into question the use of PCR positivity to count disease cases.
The study was conducted by researchers from multiple European universities and research institutes, examining data from Akkreditierte Labore in der Medizin (ALM), a laboratory consortium that conducted roughly 90% of all PCR testing in Germany during the period analyzed.
Rather than attempting to confirm individual infections through culture (showing evidence of physical, growing live virus in lab cells), the researchers compared weekly PCR-positive fractions with subsequent IgG antibody positivity, which they describe as the accepted biological marker of past infection.
“Since 1942, the detection of virus-specific antibodies has been regarded as the methodological gold standard for confirming infection.”
The logic of the analysis was straightforward.
If PCR-positive results were reliably identifying infected individuals, then PCR positivity should closely track the rise in IgG antibodies over time, given the mainstream virological and immunological model.
Instead, the researchers found that the PCR signal had to be scaled down dramatically to match observed antibody levels.
“Fitting the scaled cumulative PCR-positive fraction … yields PPCR ≈ 0.14 … This implies that roughly only one in seven German individuals with a PCR-positive test later had detectable IgG antibodies, that is, was actually infected with SARS-CoV-2.”
The article further notes that this 14% figure may still be an overestimate.
When accounting for possible testing biases, they state that the proportion of PCR positives representing real infections could be even lower.
“A more conservative interpretation of our results suggests that as few as one in eight or even in nine PCR-positive individuals … may have actually been infected.”
In other words, between 86% and 90% of PCR-positive results did not correspond to confirmed infection.
The paper emphasizes that PCR testing does not, by itself, diagnose infection.
“PCR tests merely detect the presence of fragments of viral genetic material, not necessarily an active infection.”
The study also identifies known sources of false-positive PCR results, including laboratory artifacts and statistical effects that become pronounced during mass testing.
“It is therefore important to highlight two known sources of false-positive PCR results.”
One cited example involves PCR-positive signals detected in water-only samples containing no virus at all.
“The Charité’s PCR assay produced positive results on water controls at cycle threshold (CT) values between 36 and 38.”
Beyond laboratory artifacts, the authors explain that even tests designed to be highly accurate at ruling out uninfected people can still produce large numbers of false positives when true infection levels are low.
In this context, “specificity” refers to how often a test correctly returns a negative result in someone who is not infected.
If specificity is less than 100%, some uninfected people will inevitably test positive.
“According to Bayes’ theorem, the rate of false positives increases when disease prevalence declines, owing to test specificity below 100%.”
Using observed positivity rates and their fitted infection estimate, the authors calculate that PCR specificity alone can explain the discrepancy between PCR positives and confirmed infections.
“Assuming 1% of tested individuals were true positives, a specificity of 94% explains the remaining 6% of PCR-positive results as false positives among the 99% who were not infected.”
The study’s findings have direct implications for how COVID-19 “cases” were counted and used in public policy.
Throughout the pandemic, PCR-positive test results were treated as proxies for infection and were used to justify restrictions and emergency measures.
PCR-positive test results are not being used to justify bird flu containment measures around the world.
The article argues this approach lacks biological grounding.
“A PCR-positive test alone can by no means confirm infection at the individual level.”
The paper concludes that Germany’s reliance on raw PCR positivity substantially overstated infection levels and distorted the understanding of the pandemic’s actual course.
“The principal finding from our analysis … is this: only 14%—and possibly even fewer, down to 10%—of individuals identified as SARS-CoV-2-positive via PCR testing were actually infected, as evidenced by detectable IgG antibodies.”
The article argues that PCR positivity was treated as infection when the data showed it overwhelmingly not.
By analysis, PCR positivity does not reliably indicate infection, raising questions about its continued use as a case-defining tool in current and future disease responses.
Press release admits current mRNA-based vaccine are not effective enough and contain too many impurities.
Despite mainstream attempts to downplay the alarming contamination problem plaguing COVID-19 vaccines, the Gates Foundation has awarded $3.3 million to a team of scientists at New York’s Rensselaer Polytechnic Institute (RPI) to develop “breakthrough purification technologies” for producing mRNA-based vaccines.
A September Autoimmunity study confirms that both Pfizer-BioNTech and Moderna’s mRNA COVID-19 injections contain many hundreds of times more contamination than the FDA and WHO limit.
The grant is an implicit admission that contamination is in fact a problem posed by mRNA vaccines, as well as a sign that the platform is here to stay.
Gates is funding the project because of the “impurities” and “inefficien[cy]” related to mRNA vaccines.
The research team aims to address a critical bottleneck in the production of mRNA therapeutics: the purification process that removes impurities while maintaining the integrity of the therapeutic molecule.
“This project represents a paradigm shift in how we think about mRNA purification,” Belfort said. “Current technologies are prohibitively expensive and inefficient, creating barriers to access for the populations that need them most. Our goal is to develop a purification platform that is not only more cost-effective but also more productive and scalable.”
The researchers aim to accomplish this by “replacing conventional resin-based purification systems with advanced membrane technologies and innovative binding molecules.”
The RPI announcement also admits that current mRNA-based vaccine impurities are linked to side effects and that the injectables are not effective enough, more revelations that cut against mainstream counterclaims.
Higher purity mRNA vaccines with lower immunogenic impurities could lead to improved clinical outcomes, including reduced side effects and enhanced therapeutic efficacy.
The announcement predicts the rise of self-replicating vaccine technology, which this website was the first to warn about in December 2023.
Additionally, the technology being developed could prove particularly valuable for self-amplifying RNA (saRNA) therapeutics, which require lower doses than traditional mRNA vaccines and represent the next generation of RNA-based medicines.
Gates has been developing self-copying mRNA vaccines for COVID (here, here) as well as for bird flu (here), which is the pathogen this website has been predicting will fuel the next orchestrated pandemic.
The billionaire’s latest investment is made in the name of strengthening Big Pharma infrastructure, as well as “equity” and “pandemic preparedness.”
If successful, this technology could enable local production of mRNA vaccines in regions that currently lack access to affordable biomanufacturing infrastructure, supporting global health equity and pandemic preparedness.
Despite the disease, hospitalizations, and deaths linked to mRNA jabs, the technology isn’t going anywhere.
Before injecting it into hundreds of millions of Americans via COVID-19 vaccines.
No U.S. agency has ever verified that the COVID-19 pathogen’s (SARS-CoV-2) genetic code that a Chinese government biolab supplied at the beginning of the COVID-19 pandemic—said to have been sequenced from a pneumonia patient’s lung wash—actually originated from that clinical sample before it was encoded into hundreds of millions of mRNA vaccine doses.
China never provided the physical patient sample to any U.S. institution.
In fact, Beijing issued an official directive forbidding the sharing of any samples and ordering the destruction of those samples.
And the U.S. never demanded or required an analysis of those samples before allowing its citizens to be injected with China’s pathogenic spike protein-producing code.
This critical step in verification was—and still has been—skipped, despite earlier warnings that China’s military had been exploring bioweapons development that integrates biotechnology and genetic engineering into a “new domain of warfare.”
It was also skipped despite EcoHealth Alliance’s 2018 ‘DEFUSE’ proposal to DARPA to collaborate with China to create chimeric coronavirus spike proteins with furin cleavage sites, receptor-binding domain upgrades, and two proline insertions—the defining characteristics of the COVID-19 pathogen and mRNA vaccines.
Congress, the White House, the Department of Energy, the FBI, the CIA, and Germany’s Federal Intelligence Service (BND) have confirmed that the COVID-19 pandemic was likely the result of lab-engineered pathogen manipulation—meaning billions were injected with a genetic drug that codes for a Chinese government-constructed, lab-altered spike protein.
How China Made the SARS-CoV-2 Genetic Sequence
The SARS-CoV-2 genetic code was created in a biosafety level 3 (BSL-3) laboratory at the Chinese government-run Shanghai Public Health Clinical Center, using long-debunked (here) reverse-transcription PCR (RT–PCR) technology.
Dr. Kary Mullis, the inventor of the PCR test, said in a 1997 interview (here) that his test should not be used to determine whether a patient is infected with a virus.
This is because the test “can find almost anything in anybody” if its parameters are set high enough, tainting the results.
“Anyone can test positive for practically anything with a PCR test. If you run it long enough… you can find almost anything in anybody,” he said. “It doesn’t tell you that you’re sick.”
A February 2020 Nature publication explains how China created the SARS-CoV-2 sequence:
Here we study a single patient who was a worker at the market and who was admitted to the Central Hospital of Wuhan on 26 December 2019 while experiencing a severe respiratory syndrome that included fever, dizziness and a cough. Metagenomic RNA sequencing4 of a sample of bronchoalveolar lavage fluid from the patient identified a new RNA virus strain from the family Coronaviridae, which is designated here ‘WH-Human 1’ coronavirus (and has also been referred to as ‘2019-nCoV’). Phylogenetic analysis of the complete viral genome (29,903 nucleotides) revealed that the virus was most closely related (89.1% nucleotide similarity) to a group of SARS-like coronaviruses (genus Betacoronavirus, subgenus Sarbecovirus) that had previously been found in bats in China5. This outbreak highlights the ongoing ability of viral spill-over from animals to cause severe disease in humans.
To investigate the possible aetiological agents associated with this disease, we collected bronchoalveolar lavage fluid (BALF) and performed deep meta-transcriptomic sequencing. The clinical specimen was handled in a biosafety level 3 laboratory at Shanghai Public Health Clinical Center. Total RNA was extracted from 200 μl of BALF and a meta-transcriptomic library was constructed for pair-end (150-bp reads) sequencing using an Illumina MiniSeq as previously described4,6,7,8. In total, we generated 56,565,928 sequence reads that were de novo-assembled and screened for potential aetiological agents. Of the 384,096 contigs assembled by Megahit9, the longest (30,474 nucleotides (nt)) had a high abundance and was closely related to a bat SARS-like coronavirus (CoV) isolate—bat SL-CoVZC45 (GenBank accession number MG772933)—that had previously been sampled in China, with a nucleotide identity of 89.1% (Supplementary Tables 1, 2). The genome sequence of this virus, as well as its termini, were determined and confirmed by reverse-transcription PCR (RT–PCR)10 and 5′/3′ rapid amplification of cDNA ends (RACE), respectively. This virus strain was designated as WH-Human 1 coronavirus (WHCV) (and has also been referred to as ‘2019-nCoV’) and its whole genome sequence (29,903 nt) has been assigned GenBank accession number MN908947. Remapping the RNA-sequencing data to the complete genome of WHCV resulted in an assembly of 123,613 reads, providing 99.99% genome coverage at a mean depth of 6.04× (range, 0.01–78.84×) (Extended Data Fig. 3). The viral load in the BALF sample was estimated by qPCR to be 3.95 × 108 copies per ml (Extended Data Fig. 4).
China handed the world a genetic code in computer form (in silico).
And governments all over the world accepted that code without scrutiny.
They allowed billions of people to be injected with a vaccine that creates the Chinese government’s foreign protein in the body for more than 700 days.
China Had the SARS-CoV-2 Sequence ‘More Than Two Weeks’ Before Releasing It
A January 2024 U.S. House Energy & Commerce press release confirms China possessed the SARS-CoV-2 sequence “days before the CCP acknowledged an outbreak, and more than two weeks before the China CDC release[d] their sequence.”
The congressional body said that fact “calls into question how early the CCP knew about the virus and how long they withheld this information from the world.”
This significant discovery further underscores why we cannot trust any of the so-called ‘facts’ or data provided by the CCP and calls into serious question the legitimacy of any scientific theories based on such information. The American people deserve to know the truth about the origins of SARS-CoV-2, and our investigation has uncovered numerous causes for concern, including how taxpayers’ dollars are spent, how our government’s public health agencies operate, and the need for more oversight into research grants to foreign scientists,” said Chairs Rodgers, Guthrie, and Griffith.
My report from last month revealed that before the pandemic, DARPA had developed a program to synthesize viruses purely from digital sequences within in 60 days.
Bottom Line
In the end, the world was locked down and injected on the honor system of a hostile foreign government, and not one U.S. agency has yet produced the single piece of evidence that should have come first: independent proof that China’s digital code ever came from a real human sample.
Will the same national security concern-raising strategy be used in the apparently incoming bird flu pandemic?
What follows is a documented sequence showing how the World Health Organization (WHO) seized operational control of the COVID-19 response from day one—and how it is now positioning itself to run the avian influenza pandemic the same way.
Will America follow the WHO into pandemic peril again?
The Timeline
On December 31, 2019, the Chinese government reported a cluster of pneumonia cases in Wuhan, Hubei Province.
On the same day, the WHO commandeered the international vaccine response, issuing its first “emergency use validation for a COVID-19 vaccine” emphasizing the “need for equitable global access” and declaring governments all over the world must “expedite their own regulatory approval processes to import and administer the vaccine”:
“The World Health Organization (WHO) today listed the Comirnaty COVID-19 mRNA vaccine for emergency use, making the Pfizer/BioNTech vaccine the first to receive emergency validation from WHO since the outbreak began a year ago,” reads the organization’s Dec 31 press release.
“The WHO’s Emergency Use Listing (EUL) opens the door for countries to expedite their own regulatory approval processes to import and administer the vaccine. It also enables UNICEF and the Pan-American Health Organization to procure the vaccine for distribution to countries in need.”
“‘This is a very positive step towards ensuring global access to COVID-19 vaccines. But I want to emphasize the need for an even greater global effort to achieve enough vaccine supply to meet the needs of priority populations everywhere,’ said Dr Mariângela Simão, WHO Assistant-Director General for Access to Medicines and Health Products. ‘WHO and our partners are working night and day to evaluate other vaccines that have reached safety and efficacy standards. We encourage even more developers to come forward for review and assessment. It’s vitally important that we secure the critical supply needed to serve all countries around the world and stem the pandemic.’”
“Regulatory experts convened by (the) WHO from around the world and (the) WHO’s own teams reviewed the data on the Pfizer/BioNTech vaccine.”
(The) “WHO is working to support countries in assessing their [COVID vaccine] delivery plans and preparing for use where possible.”
“The emergency use listing (EUL) procedure assesses the suitability of novel health products during public health emergencies. The objective is to make medicines, vaccines and diagnostics available as rapidly as possible to address the emergency while adhering to stringent criteria of safety, efficacy and quality.”
“Once a vaccine has been listed for WHO emergency use, WHO engages its regional regulatory networks and partners to inform national health authorities on the vaccine and its anticipated benefits based on data from clinical studies to date.”
“As part of the EUL process, the company producing the vaccine must commit to continue to generate data to enable full licensure and WHO prequalification of the vaccine. The WHO prequalification process will assess additional clinical data generated from vaccine trials and deployment on a rolling basis to ensure the vaccine meets the necessary standards of quality, safety and efficacy for broader availability.”
The very next day, January 1, 2020, the WHO set up its IMST (Incident Management Support Team), putting the organization “on an emergency footing for dealing with the outbreak,” according to the WHO’s own published timeline.
On January 5, the WHO published its first “Disease Outbreak News” on the new purported virus, which represented a “flagship technical publication to the scientific and public health community as well as global media” and gave “a risk assessment and advice” to governments, public health officials, and the mainstream international scientific community.
A Pathogen In Silico
On January 7, the Chinese government claimed to have identified a brand new coronavirus as the causative agent of the outbreak.
On January 10, China’s Center for Disease Control and Prevention (China CDC) publicly released what they said was the genetic sequence for the SARS-CoV-2 pathogen, named Wuhan-Hu-1.
The sequence was in silico only, meaning it was in a purely digital format shared on computers, as confirmed by Nature journal.
China said they produced the code from a sick man’s lung fluid using long-debunked (here) PCR technology.
Dr. Kary Mullis, the inventor of the PCR test, said in a 1997 interview (here) that his test should not be used to determine whether a patient is infected with a virus.
This is because the test “can find almost anything in anybody” if its parameters are set high enough, tainting the results.
“Anyone can test positive for practically anything with a PCR test. If you run it long enough… you can find almost anything in anybody,” he said. “It doesn’t tell you that you’re sick.”
Without any deep, long-term analysis of China’s sequence, this in silico code was accepted by governments and the international scientific community, becoming the blueprint for every coronavirus vaccine.
Billions were injected with the code, whether in the form of Pfizer and Moderna’s mRNA platform, or Johnson & Johnson’s and AstraZeneca’s immortalized-aborted-fetal-cell-based (HEK 293, PER.C6) viral vector vaccines.
Governments all over the world and Big Pharma manufacturers trusted China without question, despite warnings that China’s military had been exploring bioweapons development that integrates biotechnology and genetic engineering into a “new domain of warfare.”
No vaccinated person was given informed consent—never told these vaccines were based on a code produced by the Chinese government.
No COVID vaccine manufacturer has ever published the full genetic sequence of their COVID-19 vaccines on their own corporate websites or in standalone manufacturer-authored scientific papers.
No government or COVID vaccine manufacturer has ever published a genetic alignment between the spike protein their injections force the body to produce and the purported “wild” SARS-CoV-2 spike protein, in order to confirm the foreign protein our cells make post-vaccination is the “correct” one.
The University of Cambridge’s Medical Research Council (MRC) Toxicology Unit revealed that COVID vaccines cause the body to produce “rogue” proteins due to a “glitch” in the cellular process called ‘frameshifting,’ which stimulates an “unintended immune response in the body.”
No government or COVID vaccine manufacturer has ever published the full sequences of the plasmids used to make their injections.
Documents show that every defining structural anomaly of SARS-CoV-2—the furin cleavage site, the rebuilt human-binding motif, and the ACE-2-critical Q498 residue—matches specific pre-pandemic engineering plans and mutagenesis experiments documented in DEFUSE and earlier coronavirus manipulation studies (here, here, here, here, here).
Congress, the White House, the Department of Energy, the FBI, the CIA, and Germany’s Federal Intelligence Service (BND) have confirmed that the COVID-19 pandemic was likely the result of lab-engineered pathogen manipulation—implying billions were injected with a genetic drug that codes for a lab-altered spike protein structurally tied to the very experiments now implicated in the pandemic’s origin.
Pfizer’s own study data confirms over 1,200 diseases linked to COVID mRNA jabs, and the CDC’s Vaccine Adverse Event Reporting System (VAERS) documents 38,773 COVID-vaccine-linked deaths and 1,666,646 adverse events—though these represent fewer than 1% of actual vaccine injuries, according to a federally funded Harvard Pilgrim study.
On the same day (Jan 10), the WHO began using the phrase “2019 Novel Coronavirus” or “2019-nCoV” to refer to the disease.
WHO Rubber-Stamps China’s COVID Sequence—Big Pharma & Int’l Scientific Community Obey
On January 11, the WHO announced that it had received the Chinese government’s SARS-CoV-2 genetic sequences.
On January 12, the WHO officially endorsed China’s in silico coronavirus sequence:
“On 11 and 12 January 2020, WHO received further detailed information from the National Health Commission about the outbreak,” a press release reads.
“WHO is reassured of the quality of the ongoing investigations and the response measures implemented in Wuhan, and the commitment to share information regularly.”
Vaccine developers, including those at Moderna and Pfizer-BioNTech, initiated vaccine design within hours of the sequence becoming available, and diagnostic assays were developed within days.
The transnational scientific community accepted the sequence, leading to immediate action in diagnostics, vaccine development, and surveillance, with minimal skepticism or delay.
On January 22, the WHO convened an emergency committee to assess the outbreak.
By January 30, it declared the outbreak a Public Health Emergency of International Concern (PHEIC), advising all countries to prepare for containment, which included doomed social distancing and isolation measures, as well as the “rapid development and access” to vaccines.
WHO Declares a ‘Pandemic’
On March 11, the WHO became the first international body to officially declare the COVID-19 outbreak a global “pandemic” and, despite being a foreign and unelected body, began dictating what countries should do:
“We have called every day for countries to take urgent and aggressive action.”
Countries should “detect, test, treat, isolate, trace and mobilise their people in the response.”
“We’re calling on you to activate and scale up your emergency response mechanisms.”
“Communicate with your people about the risks and how they can protect themselves.”
“Find, isolate, test and treat every case and trace every contact.”
“Ready your hospitals, protect and train your health workers.”
“Countries must take a whole-of-government, all-of-society approach.”
“We cannot say this loudly enough or clearly enough or often enough; all countries can still change the course of this pandemic.”
“We are not suggesting to shift from containment to mitigation; we are not, we underline that.”
“All countries need to review their strategies right now.”
“Surveillance systems have to improve.”
“There’s no excuse to say that we cannot do this.”
“Countries must… take urgent and aggressive action.”
The Power & Peril of WHO-Dictated ‘Scientific Consensus’
In short, the WHO declared what would be the “scientific consensus” regarding COVID-19, and the international mainstream scientific community followed suit.
Because this mainstream supranational scientific establishment acted in lockstep with the WHO, there was no need for consent from the world’s citizenry or official government policy.
That’s the power of the WHO and internationally curated “scientific consensus,” no matter how fabricated and fraudulent that consensus might be.
The COVID pandemic proved that the WHO and scientific community—an infinitesimally small group of elite multinational agents—can make the world bend to their will.
After its two-year investigation into the COVID-19 pandemic, the Congressional Select Subcommittee on the Coronavirus Pandemic confirmed that the WHO’s draconian authoritarianism throughout the pandemic “was an abject failure,” writing:
“The WHO’s response to the COVID-19 pandemic was an abject failure because it caved to pressure from the Chinese Communist Party and placed China’s political interests ahead of its international duties. Further, the WHO’s newest effort to solve the problems exacerbated by the COVID-19 pandemic—via a “Pandemic Treaty”—may harm the United States.”
But there is no need for a treaty, no matter how national-sovereignty-degrading, when the world’s public health leaders and self-appointed scientific elite unquestioningly carry out the WHO’s bidding.
Bottom Line
The WHO is right now orchestrating a coming avian influenza “bird flu” pandemic.
Simultaneously, governments all over the world are performing reverse-genetics gain-of-function (GOF) experiments on- and developing countermeasures (vaccines, etc.) for bird flu (see links below).
Just as they were before the COVID pandemic.
The Trump administration has been “actively participating” in WHO bird flu seminars despite the president’s January 2025 executive order to withdraw from the organization.
The admin’s $500 million ‘Generation Gold Standard’ platform is focused on bird flu vaccine development.
If the WHO repeats its COVID plan with avian influenza, we will see the same rapid lockstep activation of a prebuilt command system—instant acceptance of an unverified digital genome, accelerated vaccine deployment, suppressed dissent, and a global population maneuvered once again into mandatory genetic countermeasures before independent validation is possible.
U.S. officials and American citizens must decide now whether they will permit this system to run again, or whether they will finally impose the oversight and resistance that were absent the first time.
Unelected foreign body believes coronavirus still has the “capacity to trigger epidemics and pandemics.”
The World Health Organization (WHO) has released a “new strategic plan for the management of coronavirus disease threats,” according to a Wednesday press release.
The announcement comes after the WHO, with Gates Foundation funding, published its blueprint for a supranational digital ID system that tracks every person on Earth from birth, merges vaccine status with income, ethnicity, and religion, and deploys AI-driven surveillance to identify, target, and monitor entire populations.
Per today’s press release, the WHO wants to control how sovereign nations respond to “COVID-19, Middle East respiratory syndrome (MERS), and potential new coronavirus diseases.”
The plan “encompasses both routine management as well as emergency scenarios” involving the “emergence of a new coronavirus with pandemic potential.”
The unelected international foreign body emphasizes that the move represents “the first such unified plan.”
The goal is “sustained, long-term, and integrated management.”
WHO says it’s doing this in the name of “advancing integration, sustainability, and equity,” common globalist-tied tropes.
The plan is part of the organization’s “2025–2030” agenda for national health authorities to participate in an “action-oriented approach to managing coronavirus disease threats in the broader context of infectious disease management.”
WHO’s justification is the coronavirus’s alleged “capacity to trigger epidemics and pandemics.”
WHO insists that “uncertainties persist around virus evolution and long-term impacts of COVID-19.”
One WHO director explained that the plan also lumps in efforts regarding influenza, the pathogen that this website has been warning readers is currently being dangerously manipulated in government-funded laboratories all over the world.
The director urged government leaders to prepare for “future” pathogenic threats by falling in line with the WHO:
“Coronaviruses remain one of the most consequential infectious disease threats today,” said Dr Maria Van Kerkhove, WHO Acting Director for Epidemic and Pandemic Management. “Integrating their management into broader respiratory disease and infectious threat prevention and control programmes, including for influenza, is essential. While each country will have its own approach tailored to its national context, WHO urges Member States to use the strategic directions set out in the plan to build resilient health systems that can effectively manage current threats while preparing for future ones.”
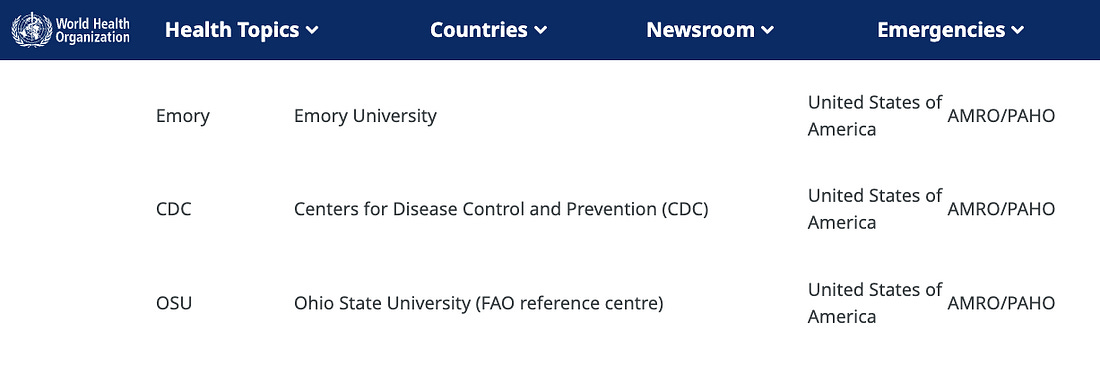
The WHO is expanding its CoViNet “sentinel surveillance” network, now comprised of 45 laboratories.
Eleven labs were added this year alone, signifying the magnitude of the operation.
“To strengthen global coronavirus monitoring, WHO has also expanded its Coronavirus Network (CoViNet), a network of disease surveillance programmes and reference laboratories for SARS-CoV-2, MERS-CoV, and emerging coronaviruses of public health significance. CoViNet now includes 45 national reference laboratories across the human, animal, and environmental health sectors, with 11 laboratories added in 2025. CoViNet complements WHO’s Global Influenza Surveillance and Response System (GISRS), which conducts global sentinel surveillance, including for SARS-CoV-2.”
Despite President Donald Trump’s January executive order withdrawing the U.S. from the WHO, CoViNet includes labs belonging to Emory University, Ohio State University, and the Centers for Disease Control and Prevention (CDC).
In short, the WHO’s new “strategic plan” represents an international effort to centralize pandemic authority under an unelected foreign body, erode national sovereignty, override accountability, and collapse public-health decision-making into a global command structure.
And it comes even after President Trump formally withdrew the United States from the WHO, underscoring how deeply these surveillance and biosecurity networks remain embedded—and how ripe they are for further abuse.
No one who understands the politics of ‘the science’ trusts it or will allow a gene therapy bioweapon into their bodies or of those they love and care for. Why are these shots still available?
Aussie17 writes a great blog. Below is posted Part 1 of his [?]/her [?] vitally important and compelling 2-part series linking the COVID jabs, through clean, reliable data from Singapore, with the one and only medication for a previously rare, devastating, invariably fatal disease called Amyotrophic Lateral Sclerosis (ALS).
There is only one use for the particular drug followed in the stack: ALS. Since the people taking it are ALS patients who have a short lifespan, if more is sold because more people are taking it. That can only be because more people have ALS. Q: Why do more people have ALS, decreased fertility, auto immune diseases, turbo cancer and excess death? A: ABTS [Anything but the shots]
It is urged that you read these two pieces and do several things: first, commit to being the voice of truth about these indescribably dangerous weapons against humanity disguised as “vaccines”. They are not. And clean statistics from around the world make that horrifyingly clear. Only governments and their lackies can find any way to deny this. It is up to us, all of us, to amplify this message.
Second, commit to doing whatever is necessary to protect your own body and that of people you have control over (parents for minor children, for example).
That means never, ever [again?] permit this or any other “untested” government-provided miracle snake oil substance into your body (or theirs).
Third, in order to educate yourself, and check out the idea that every aspect of our lives is already permeated by the United Nations parasite, perform this quick experiment: using the search engine of your choice, enter the following (filling in the blank with your town or agency impacting your profession or State or Province or country): ” List, with references and links, all of the UN-derived, UN-compliant, UN-related or UN-adjacent programs, policies, protocols, policies and partnerships which impact directly or indirectly [fill in the blank].”
It is promised that that your jaw will be somewhere in the vicinity of your knees when you see what comes back.
Now here is Part 1 of Aussie17’s important correlation of deeply meaningful information:
A big part of Big Pharma is spinning a good story around sales numbers for the bosses. Nail the narrative, and you’re golden for another year. Botch it, and you’re packing your desk.
Why is this important? Well, for quite a few reasons, but a big one is because, especially in light of Dr. Prasad’s letter acknowledging that Covid jabs kill kids, with the mRNA shots still on the market and new mRNA jabs, including the uber-deadly replicon shots, being approved all the time, especially for kids (and, thanks to Merck, for your pets, too), we are dealing with weak-kneed damage control, not the beneficent or beneficial regulatory service to the public. We pay for regulation, not rubber-stamped death and disease but that is what we get.
Doin’ the Ol’ “HHS is Here for You, Regulating to Protect Your Health, Bobby Kennedy’s Our Guy” Rag
Let it be clear: Bobby knows full well that mRNA jabs are bioweapons. Prasad knows. Bhattacharya knows. There is, and has never been, a dearth of knowledge of how deadly these shots are. Pfizer and Moderna know. So does the Department of Defense. Anyone who genuinely cares about ending the REAL pandemic, not the COVID propagandemic nonsense, but the deadly reality of the medical murders and the public health harms and, most of all, the bioweapon jabs, would not play nice, bide his time and be a good politician. He would move heaven and earth to end the deadly scourge of gene editing, death dealing weapons killing and maiming us while they destroy our ability to reproduce humankind.
Or he could pretend to be working on it and not accomplish anything even coming close to protecting the public from the bioweapon.
Hey, Mr. Secretary (and Mr. President), did you get caught with your regulatory pants down? Well, just keep on doing what you have done for nearly a year: pretend you are doing performance art and you really meant to be in that awkward position and indicate how much thought went into getting your rear end exposed.
That’s the science we are supposed to trust, after all. And we had that revelation about autism to trust, too. Now that was some seriously trustworthy science, right?
Then, because the public let you get away with that, you can just keep on doing more of same, right?
But don’t, for God’s sake, waste all the time and money and creativity that has gone into this decades long, untold trillions of dollars’ worth of bioweapon program by interfering with it! No, Siree Bob! Cover your tracks first, lie out of every orifice you and your associates can make any sounds out and keep the bioweapons in the rapid approval pipeline.
Most important of all, of course, cover your own ass if you can manage it, and keep on doing what you’re doing.
Maybe nobody will notice while they are exterminated from the bioweapons on the shelves and in the clinics.
Or maybe we will. And maybe we will eject the deadly UN parasite from every cell in the Body Politic and make some real headway to recovery
Nothing less.
And neither the head of the Executive Branch of the US government nor his appointee over at Health and Human Services has done so. Meanwhile, we suffer and die through an entirely man-made plague.
As it turns out, hiding it in Singapore is quite difficult. Thus, this outstanding two-part revelation.
Who is behind it? The genocidal maniacs who think you and I are disposable at their whim and pleasure. That’s right: the globalist parasites who operate the United Nations for their pleasure and profit, and for our pain and punishment. We, after all, are the carbon they intend to eliminate.
The solution? a good, comprehensive detox to get the UN and its bits and pieces out of our lives, our bodies, our government, our schools, our town halls, our clinics and hospitals, our airports, our banks and everywhere else.
























Recent Comments